Wondering whether the numbers you saw on a recent echo mean anything serious? In a nutshell, a healthy pulmonary artery systolic pressure is usually20mmHg, the mean pressure hovers around1216mmHg, and the diastolic pressure sits near810mmHg. If your values tip beyond these limits, it might be a gentle nudge from your body to look a bit closer at your hearts right side.
Why does this matter? Because the pulmonary artery is the highway that carries blood from the heart to the lungs. When pressure climbs on that road, the heart has to work harder, and over time this can lead to pulmonary hypertensiona condition thats manageable when caught early, but tricky if ignored. If you or a family member are dealing with symptoms after a valve procedure, resources on heart valve recovery can help explain how recovery and pressures interact.
Quick answer summary
Is my pulmonary artery pressure normal?
At rest, most healthy adults have a pulmonary artery systolic pressure (sPAP) of20mmHg, a mean pulmonary artery pressure (mPAP) of roughly1216mmHg, and a diastolic pressure (dPAP) of about810mmHg. These ranges are widely accepted in cardiology textbooks and echo labs. If your recent test shows a systolic reading of 35mmHg, for instance, thats above the normal range and merits further conversation with your clinician.
Why does it matter?
Elevated pressure can be a silent sign that somethings amissperhaps chronic lung disease, leftheart problems, or earlystage pulmonary hypertension. The good news is that, when identified early, lifestyle tweaks, medications, and targeted therapies can keep the numbers in check and protect your hearts longterm health.
How pressure measured
Invasive methods
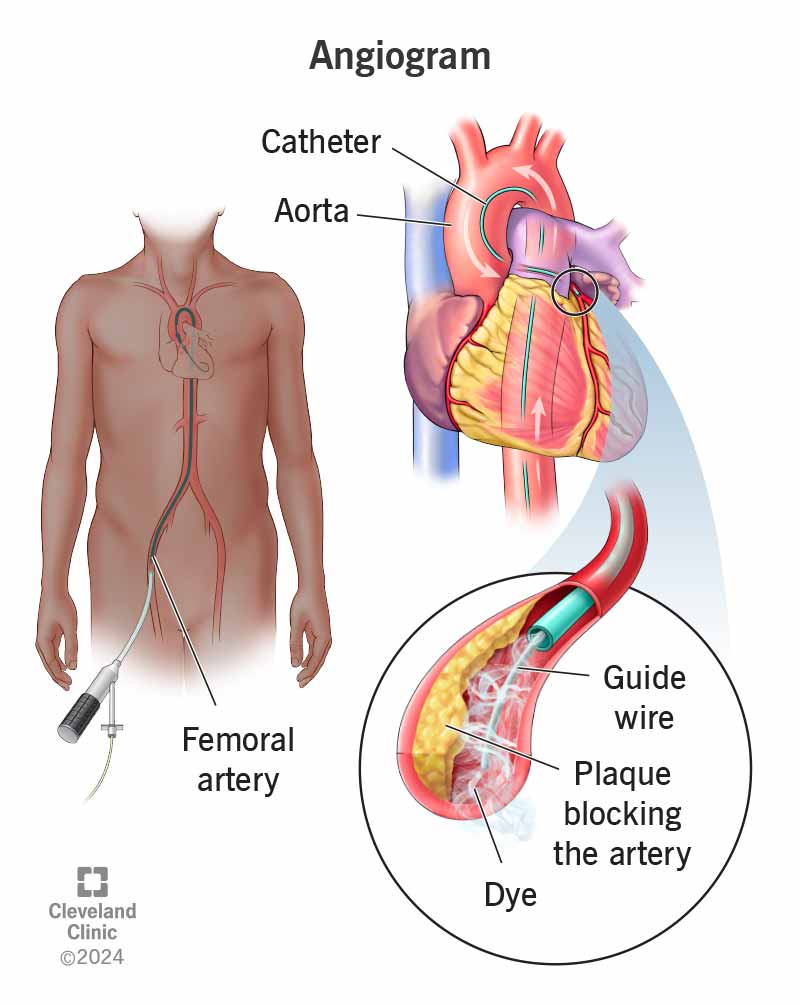
The goldstandard way to get an exact pressure reading is a rightheart catheterisation. A thin, flexible tube is threaded through a vein (usually in the neck or groin) and guided into the right side of the heart and pulmonary artery. While it sounds a bit intimidating, most patients describe the experience as a brief quick poke followed by a short monitoring period. The procedure provides direct, beatbybeat pressure data and can also assess how the lungs and heart respond to medication on the spot.
Stepbystep of a catheter study
1. Preparation Youll fast for a few hours and may receive a mild sedative to keep you comfortable.
2. Access A local anesthetic numbs the insertion site; a sheath is placed into the vein.
3. Navigation Using Xray guidance, the cardiologist threads the catheter into the right atrium, right ventricle, and finally the pulmonary artery.
4. Measurement Realtime pressure tracings appear on the monitor; the team records systolic, diastolic, and mean values.
5. Completion The catheter is withdrawn, pressure is applied to the site, and youre usually discharged the same day.
Noninvasive estimates
Most people never need a catheter. Instead, doctors rely on transthoracic echocardiography (TTE), a painless ultrasound of the heart. By measuring the speed of blood flowing through the tricuspid valve, the echo can calculate an estimated sPAP using the Bernoulli equation. While not as precise as a catheter, modern echo machines are remarkably accurate, especially when performed by experienced sonographers.
Sample echo report snippet
Estimated systolic pulmonary artery pressure: 28mmHg (based on tricuspid regurgitant jet velocity 2.5m/s). No evidence of rightventricular overload. This kind of line appears in a typical echo report and gives you a quick snapshot of where you stand.
Normal pressure ranges
Mean pulmonary artery pressure
The mPAP reflects the average pressure throughout the cardiac cycle. In healthy adults it usually falls between 12mmHg and 16mmHg, with many textbooks quoting an average of 143mmHg. This value is crucial because recent guidelines from the European Society of Cardiology define pulmonary hypertension as an mPAP20mmHga modest shift from the older 25mmHg cutoff, highlighting how sensitive modern medicine has become to early changes.
Systolic pulmonary artery pressure
When you hear pulmonary artery pressure, most people think of the systolic number. A systolic pressure 20mmHg is considered normal at rest. Some sources provide a slightly broader upper normal window of 1825mmHg, but anything above 30mmHg generally prompts further evaluation.
Diastolic pulmonary artery pressure
The diastolic reading tells us how the vessel behaves when the heart relaxes. Normal dPAP values sit comfortably between 8mmHg and 10mmHg, though a range of 612mmHg is often quoted to accommodate individual variability.
Comparison table
| Parameter | Normal Range | Typical Upper Limit (Clinical Concern) |
|---|---|---|
| Mean Pulmonary Artery Pressure (mPAP) | 1216mmHg | 20mmHg (pulmonary hypertension) |
| Systolic Pulmonary Artery Pressure (sPAP) | 20mmHg | 35mmHg (mild elevation) |
| Diastolic Pulmonary Artery Pressure (dPAP) | 810mmHg | 15mmHg (significant rise) |
When pressure high
Pulmonary hypertension definition
According to the 2022 ESC/ERS guidelines, pulmonary hypertension is diagnosed when the mean pulmonary artery pressure is 20mmHg or higher at rest, measured by rightheart catheterisation. This lower threshold reflects newer research showing that even modest pressure increases can affect exercise capacity and quality of life.
Pressure categories
Clinicians often break down elevated pressures into three handy buckets:
- 35mmHg systolic Mild elevation; many patients feel fine, but a deeper look is warranted.
- 40mmHg systolic Moderate rise; usually triggers additional testing (e.g., pulmonary function tests, CT angiography).
- 50mmHg systolic Severe elevation; urgent referral to a pulmonary hypertension specialist is recommended.
Case vignette
Meet Sarah, a 55yearold avid hiker who went for a routine health check. Her echo showed an estimated sPAP of 38mmHg. Though she felt mostly fine, the slight breathlessness on steep climbs nudged her doctor to order a full rightheart catheter study. The results confirmed a mean pressure of 22mmHgjust over the new threshold. With a combination of lowdose sildenafil and a structured exercise plan, Sarahs pressures dropped back into the lownormal range within six months, and shes back on the trail, enjoying the view.
Factors affecting pressure
Physiological influences
Even in perfectly healthy people, a few everyday factors can nudge pulmonary pressures higher or lower:
- Age Vascular stiffness rises with age, modestly increasing sPAP.
- Body mass index (BMI) Obesity can elevate pressures by amplifying blood volume and respiratory drive.
- Altitude Higher elevations reduce oxygen, prompting the lungs to constrict their vessels and raise pressure.
- Exercise Intense aerobic activity temporarily spikes systolic pressure; regular training, however, tends to lower resting values.
Pathological influences
When something goes wrong in the lungs or left side of the heart, the right side has to compensate, pushing the pulmonary artery pressure up:
- Chronic obstructive pulmonary disease (COPD) Airway obstruction leads to hypoxic vasoconstriction.
- Interstitial lung disease Fibrotic tissue stiffens the lungs, raising resistance.
- Leftheart disease If the left ventricle backs up blood, pressure travels backward into the pulmonary circulation.
- Chronic thromboembolic disease Unresolved clots block pulmonary vessels.
Quicklook checklist
| Risk Factor | Potential Impact on Pressure |
|---|---|
| Age>60y | Modest in sPAP |
| BMI30kg/m | blood volume pressures |
| Living >2,500m altitude | Hypoxiadriven vasoconstriction |
| History of COPD | Chronic pulmonary vascular resistance |
| Leftsided heart failure | Backward pressure transmission |
Next steps checklist
When to see a doctor
If any of the following sound familiar, its time to pick up the phone:
- Unexplained shortness of breath, especially during mild activity.
- Persistent fatigue or feeling out of breath after climbing a single flight of stairs.
- Swelling in the ankles or lower legs.
- Chest discomfort that isnt classic heartattack pain but feels tight when you exert yourself.
- Recent echocardiogram showing a systolic pressure35mmHg.
Preparing for a test
Before you head to the cardiology clinic, a few simple steps can smooth the process:
- Write down any medications (including overthecounter supplements) youre taking.
- Note the time of your last meal; many labs ask you to fast for a few hours.
- Bring a list of symptoms, their onset, and anything that makes them better or worse.
- Prepare a few questions in advanceWhat does my sPAP of 38mmHg mean for my daily life? is a great starter.
Printable log template
| Date | Resting O Sat (%) | Symptoms | Notes (meds, activity) |
|---|---|---|---|
| 20250801 | 96 | Mild breathlessness on stairs | Morning inhaler, no exercise |
| 20250808 | 98 | None | Walked 30min, no meds |
Conclusion
Understanding the pulmonary artery pressure normal range isnt just a numbers gameits a roadmap that helps you spot early warning signs, make informed lifestyle choices, and partner effectively with your healthcare team. Remember, a systolic pressure20mmHg, mean pressure1216mmHg, and diastolic pressure810mmHg are the sweet spots most of us aim for. If you notice anything off, dont waitreach out, get a proper echo, and discuss the next steps with a trusted clinician. Feel free to download the quickreference checklist above, share your own experiences in the comments, or ask any lingering questions. Were all in this together, and knowledge is the best medicine.
FAQs
What is considered a normal pulmonary artery pressure?
At rest, a healthy adult typically has a systolic pressure ≤ 20 mm Hg, a mean pressure of 12‑16 mm Hg, and a diastolic pressure of 8‑10 mm Hg.
How is pulmonary artery pressure measured without a catheter?
Most clinicians use transthoracic echocardiography (TTE) to estimate systolic pressure from the tricuspid regurgitant jet velocity using the Bernoulli equation.
When should I be concerned about elevated pulmonary artery pressure?
Persistent systolic readings ≥ 35 mm Hg, a mean pressure ≥ 20 mm Hg, or symptoms such as unexplained shortness of breath, fatigue, or leg swelling warrant further evaluation.
What conditions can raise pulmonary artery pressure?
Common causes include chronic lung diseases (e.g., COPD, interstitial lung disease), left‑heart failure, chronic thromboembolic disease, and certain forms of pulmonary hypertension.
What are the next steps if my echo shows a high pressure estimate?
Your doctor may order additional testing such as pulmonary function tests, CT angiography, or a right‑heart catheterisation to confirm the diagnosis and guide treatment.