If your heart and kidneys start talking to each other in the wrong way, youll quickly feel the ripple effect a little swelling here, a sudden rise in blood pressure there, and the whole system feels out of sync. In plain words,cardiorenal syndromeis when a problem in the heart harms the kidneys, or a kidney issue harms the heart, and doctors sort it into five distinct types.
Knowing which type youre dealing with (type15) is the shortcut to the right treatment plan, realistic expectations about lifeexpectancy, and the tests that actually matter. Below, we walk through each type, how its diagnosed, and what the latest evidence says about managing it. Grab a cup of tea, settle in, and lets demystify this together.
Quick Overview
Heres a rapid snapshot of the fivecardiorenal syndrome types:
- Type1 Acute Cardiorenal (heart kidney)
- Type2 Chronic Cardiorenal (heart kidney)
- Type3 Acute Renocardiac (kidney heart)
- Type4 Chronic Renocardiac (kidney heart)
- Type5 Secondary (systemic) (both organs injured by a common disease)
If youd like a printable cheatsheet, you can download our cardiorenal syndrome types PDF its a handy reference for clinicians and patients alike.
Type One Explained
What Is Cardiorenal Syndrome Type 1?
Pathophysiology
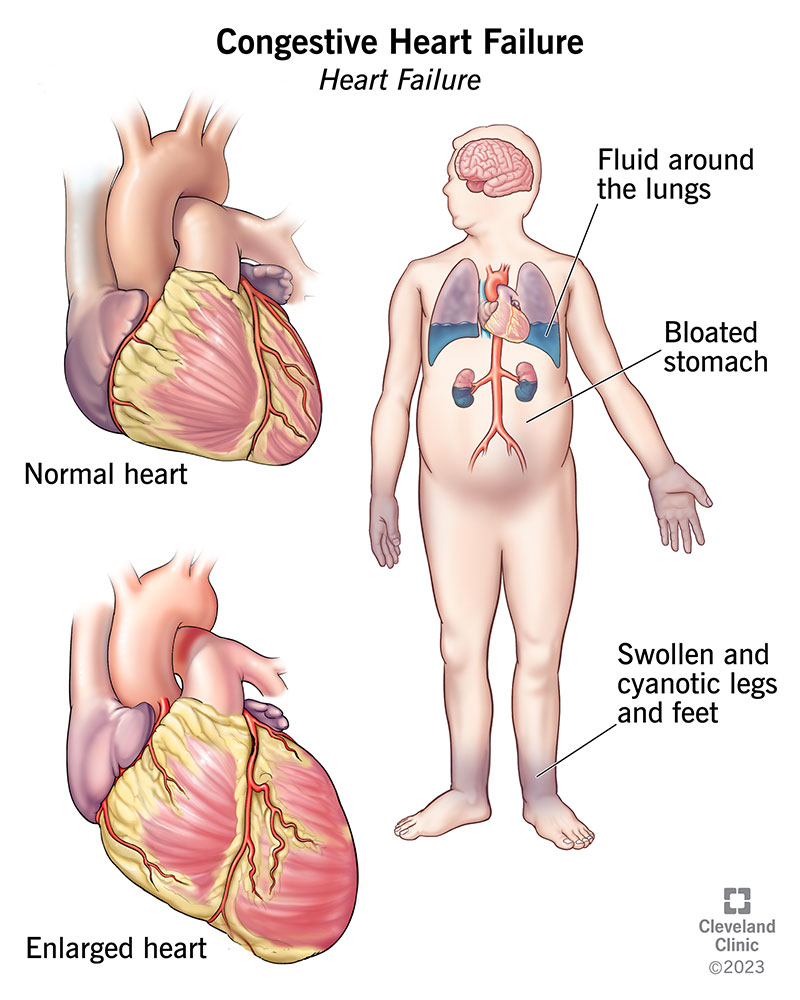
Type1, also called acute cardiorenal syndrome, is the sudden spillover of a heart crisis into the kidneys. When the left ventricle cant pump efficiently, pressure backs up into the veins, reducing renal perfusion and triggering a cascade of neurohormonal activation (RAAS, sympathetic surge). In short, the kidneys get starved of blood and react by holding onto fluid, which only makes the heart work harder a vicious loop.
Typical Clinical Signs & Red Flags
- Rapid rise in serum creatinine (often >0.3mg/dL within 48hours)
- New onset oliguria or sudden weight gain
- Worsening dyspnea and pulmonary edema
- Elevated BNP or NTproBNP levels
Diagnostic Criteria
According to the , a rise in creatinine of 0.3mg/dL within 48hours or a 50% decrease in eGFR qualifies, provided it follows an acute cardiac event such as decompensated heart failure.
FirstLine Treatment Options
- Stabilize hemodynamics gentle diuretics to relieve congestion, vasodilators if blood pressure permits.
- Introduce cardioprotective drugs early (lowdose ACEinhibitor or ARNI, and consider an SGLT2 inhibitor for renal protection).
- Monitor electrolytes and fluid balance closely; avoid nephrotoxic agents.
RealWorld Example
John, a 62yearold with chronic hypertension, was admitted for acute decompensated heart failure. Within 24hours, his creatinine climbed from 0.9 to 2.1mg/dL. After adjusting his diuretic regimen and initiating an ARNI, his kidney function stabilized and he was discharged two weeks later.
Type Two Explained
What Is Cardiorenal Syndrome Type 2?
Pathophysiology
Type2 is the longterm partner of type1. Chronic heart failure leads to persistent low cardiac output and elevated venous pressures, gradually impairing renal perfusion. Over months to years, the kidneys develop chronic kidney disease (CKD) as they adapt to the constant lowflow state.
Symptoms & LongTerm Risks
- Gradual fatigue and exercise intolerance
- Persistent peripheral edema
- Slowly declining eGFR, often unnoticed until a routine labs draw shows a dip
- Anemia and bonemineral disturbances common in CKD
Diagnostic Workup
The key is to confirm both chronic heart failure (NYHA classIII/IV) and a sustained eGFR<60ml/min/1.73m for at least three months. Echocardiography, BNP testing, and serial creatinine measurements are the standard trio.
Treatment & Lifestyle Management
Guidelinedirected heartfailure therapy is the cornerstone: ACEinhibitor/ARNI, betablocker, mineralocorticoid receptor antagonist, and, increasingly, SGLT2 inhibitors (theyve shown a 3040% reduction in renal decline in recent trials). Dietary sodium restriction, regular physical activity within tolerance, and vigilant blood pressure control round out the plan.
Patient Story
Maria, 70, was diagnosed with type2 after her cardiologist noticed a subtle rise in creatinine during a routine visit. By adding dapagliflozin to her regimen and tightening her sodium intake, her eGFR held steady for three yearsa win for both heart and kidneys.
Type Three Explained
What Is Cardiorenal Syndrome Type 3?
Pathophysiology
Here the kidney initiates the drama. An acute kidney injury (AKI) releases excess fluid, uremic toxins, and electrolyte imbalances into the bloodstream, which can precipitate arrhythmias, myocardial stunning, and sudden heart failure. Think of the kidneys overloading the heart with too much water and waste.
Clinical Clues
- Newonset atrial fibrillation or ventricular tachyarrhythmia after a bout of AKI
- Rapid increase in troponin unrelated to coronary artery disease
- Pulmonary congestion developing within days of a contrastinduced AKI
Diagnosis Checklist
Identify AKI based on KDIGO staging (stage2/3) and then look for evidence of new cardiac dysfunction (echocardiographic decline, elevated troponin, or clinical heart failure) within seven days.
Management Strategies
- Address the renal insult promptly stop nephrotoxic drugs, manage volume status, and consider early renal replacement therapy if indicated.
- Control electrolytes (especially potassium and magnesium) to avoid arrhythmias.
- Treat the cardiac fallout with inotropes or afterload reducers, guided by hemodynamic monitoring.
Example Scenario
After a complicated abdominal surgery, Mr. Patel developed a contrastinduced AKI (creatinine rose from 0.8 to 2.5mg/dL). Within 48hours, he presented with shortness of breath and a new leftbundlebranch block. Prompt dialysis, diuretic adjustment, and lowdose dobutamine stabilized both his kidneys and heart.
Type Four Explained
What Is Cardiorenal Syndrome Type 4?
Pathophysiology
Chronic kidney disease (CKD) can be a silent assassin for the heart. Longstanding hypertension, anemia, and the buildup of uremic toxins promote leftventricular hypertrophy and diastolic dysfunction. The heart must work harder to pump against stiff arteries and an overloaded circulatory system.
Hallmarks & Monitoring
- Progressive leftventricular hypertrophy on echocardiography
- Elevated BNP despite stable kidney function
- Worsening diastolic parameters (E/e ratio increase)
EvidenceBased Treatment
Blood pressure control is paramount target <130/80mmHg. Use ACEinhibitors or ARBs, and add a mineralocorticoid receptor antagonist when appropriate. Recent data show SGLT2 inhibitors (e.g., empagliflozin) cut cardiovascular events in CKD patients, even without diabetes.
Case Highlight
Sarah, 58, with stage3 CKD, began experiencing fatigue and mild dyspnea. An echo revealed concentric LVH. After initiating a lowdose ACEinhibitor and dapagliflozin, her symptoms improved, and her ejection fraction held steady over two years.
Type Five Explained
What Is Cardiorenal Syndrome Type 5?
Definition & Triggers
Type5 is the systemic form a single disease (sepsis, systemic lupus erythematosus, diabetes, etc.) damages both heart and kidneys simultaneously. The injury isnt a domino effect but a parallel assault.
Typical Presentations
- Multiorgan failure in the intensive care unit
- Simultaneous rise in troponin and creatinine
- Inflammatory markers (CRP, ferritin) markedly elevated
Diagnostic Approach
Confirm the underlying systemic disease (blood cultures for sepsis, autoantibody panels for SLE, HbA1c for uncontrolled diabetes) and document concurrent cardiac and renal injury using biomarkers and imaging.
Integrated Treatment Plan
- Target the root cause antibiotics for sepsis, immunosuppression for autoimmune flare, tight glucose control for diabetes.
- Provide organsupportive care cautious fluid management, early renal replacement therapy if needed, and inotropes for cardiac support.
- Engage a multidisciplinary team (cardiology, nephrology, critical care) to synchronize therapy.
RealWorld Example
A 45yearold admitted with septic shock from a perforated ulcer showed a creatinine climb to 3.2mg/dL and a troponin rise to 1.5ng/mL within 12hours. Early broadspectrum antibiotics, source control surgery, lowdose norepinephrine, and continuous renal replacement therapy turned the tide, and he was discharged home after three weeks.
Comparison Table
| Type | Primary Origin | Time Course | Typical Trigger | Key Diagnostic Marker | FirstLine Therapy |
|---|---|---|---|---|---|
| 1 | Heart Kidney | Acute | Acute decompensated HF | Creatinine 0.3mg/dL 48h | Diuretics + ACEi/ARNI |
| 2 | Heart Kidney | Chronic | Chronic HF (NYHAIII/IV) | Persistent eGFR<60 | Guidelinedirected HF meds |
| 3 | Kidney Heart | Acute | AKI (contrast, sepsis) | New LV dysfunction 7days | Volume control + RRT |
| 4 | Kidney Heart | Chronic | CKD stage35 | LVH, diastolic dysfunction | BP control, SGLT2i |
| 5 | Systemic | Both | Sepsis, SLE, diabetes | Dual biomarker rise | Treat underlying disease + organ support |
Practical Takeaways
1. Identify the type early. The sooner you know whether youre looking at an acute heartdriven problem or a chronic kidneydriven one, the quicker you can start the right therapy.
2. Use the diagnostic criteria. Rely on established cardiorenal syndrome diagnostic criteria rather than guesswork it improves outcomes and reduces unnecessary testing.
3. Treat both organs. Ignoring the other organ is a common pitfall. Even a modest ACEinhibitor dose can protect kidneys while helping the heart.
4. Stay updated on emerging therapies. SGLT2 inhibitors, once a diabetes drug, are now a cornerstone for manycardiorenal syndromepatients, regardless of blood sugar levels.
5. Download the cheatsheet. For a quick reference on cardiorenal syndrome types PDF, click the link above its perfect for clinicians, caregivers, and anyone wanting a clear snapshot.
Conclusion
Understanding the fivecardiorenal syndrome types is more than an academic exercise; its a practical roadmap that guides treatment, sets realistic expectations about life expectancy, and empowers you to take charge of your health. By spotting whether the heart or the kidneys started the trouble and whether its an acute flare or a chronic march you can aim for targeted therapies, monitor the right labs, and work with a multidisciplinary team to keep both organs humming. If you have questions, need clarification on a specific type, or want to discuss the latest treatment options, feel free to reach out to your healthcare provider. Knowledge is the best medicine, and together we can navigate this complex partnership with confidence.