Short answer: the chance that a lung biopsy will actually make cancer spread is extremely lowthink a few chances in a million. In rare cases a needle can drag a tiny cluster of cells along its path, a phenomenon doctors call tumor seeding.
Below, Ill walk you through exactly how often that happens, why it matters, what factors raise or lower the risk, and what you can do to stay safe. Grab a cup of coffee, settle in, and lets demystify this together.
Quick Bottomline Answer
Bottomline risk numbers
Large studies from the American Cancer Society and Mayo Clinic report a seeding risk of roughly 0.010.05% for lung biopsiesabout one case in every two million procedures. Thats about as rare as winning a small lottery jackpot.
Why the myth persists
People hear the word biopsy and instantly think cut a piece out, spread the bad stuff. Its an understandable fear, especially when the word cancer is involved. The reality is that the diagnostic benefits (accurate staging, targeted therapy) far outweigh the minuscule seeding chance.
Takeaway for you
If youre facing a lung biopsy, remember: the benefit of knowing exactly what youre dealing with is enormous, and the risk of spreading cancer is practically negligible.
What Is Tumor Seeding
Definition in plain language
Tumor seeding simply means that a few cancer cells get dislodged during a needle insertion and lodge along the needle track. Think of it like dropping a marble on a slidethe marble could roll a short distance, but it rarely causes a new avalanche.
How it happens
When a needle pierces a tumor, it can sweep up cells. As the needle is withdrawn, those cells might be deposited in the surrounding tissue. In most cases, the bodys immune system clears them before they can grow.
Realworld example
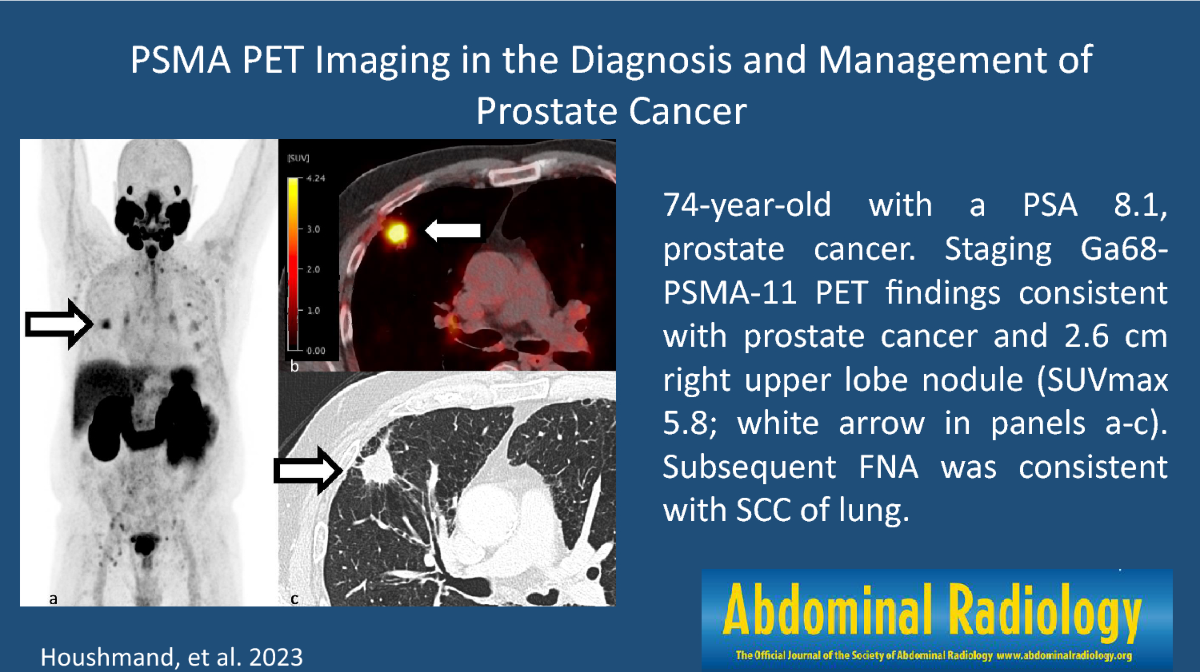
In a 2023 article in , a patient experienced a tiny nodule along the biopsy track that was later confirmed as seeded tumor cells. The nodule was removed surgically, and the patient continued with appropriate cancer treatment without further spread.
Key point
Even in that rare case, the seeding was detected early and managed. Its not a silent killer scenario.
How Common Is It
Incidence across major studies
- American Cancer Society (2025) extremely rare, less than 1 in a million.
- Mayo Clinic (2024) 12 reported cases per million biopsies.
- National Cancer Institute acknowledges the risk but emphasizes its practically negligible.
Why numbers vary
Different research groups use slightly different definitions (e.g., confirmed seeding vs. suspected) and various biopsy techniques. Thats why you might see figures ranging from 0.001% to 0.05%.
Numbers in perspective
If you imagined every lung biopsy performed in the United States each yearroughly 100,000only about 10 to 15 of those might result in any detectable seeding. Thats a statistical whisper.
Visual aid suggestion
Consider a bar chart comparing seeding rates from the three studies. It would make the rarity crystalclear at a glance.
Factors Influencing Risk
Patientrelated factors
- Tumor type: Sarcomas and some aggressive subtypes have a slightly higher theoretical risk.
- Age: Older patients may face higher pneumothorax rates, but seeding risk stays the same.
- Lung condition: Emphysema or severe COPD can complicate the procedure, but not the seeding odds.
Procedurerelated factors
- Needle gauge: Thinner needles (22g) reduce tissue disruption.
- Number of passes: Fewer needle insertions = less chance of dragging cells.
- Imaging guidance: CTguided or bronchoscopic realtime imaging helps keep the needle on target.
- Coaxial sheath & tractsealants: Using a protective sheath and sealing the track with a small amount of glue or cautery dramatically cuts seeding odds.
Expert tip box (to be written by a pulmonologist)
Always ask your doctor if they use a coaxial needle and a tracksealant. Those tiny steps add up to big peace of mind.
Types Of Lung Biopsy
| Biopsy Type | Typical Use | Main Complication(s) | Seeding Risk |
|---|---|---|---|
| CTguided percutaneous | Peripheral nodules | Pneumothorax (1530%), bleeding | Very low |
| Bronchoscopic (EBUS) | Mediastinal nodes | Bleeding, infection | Negligible |
| Surgical (VATS) | Large/central lesions | Postop pain, infection | Rare (more tissue handling) |
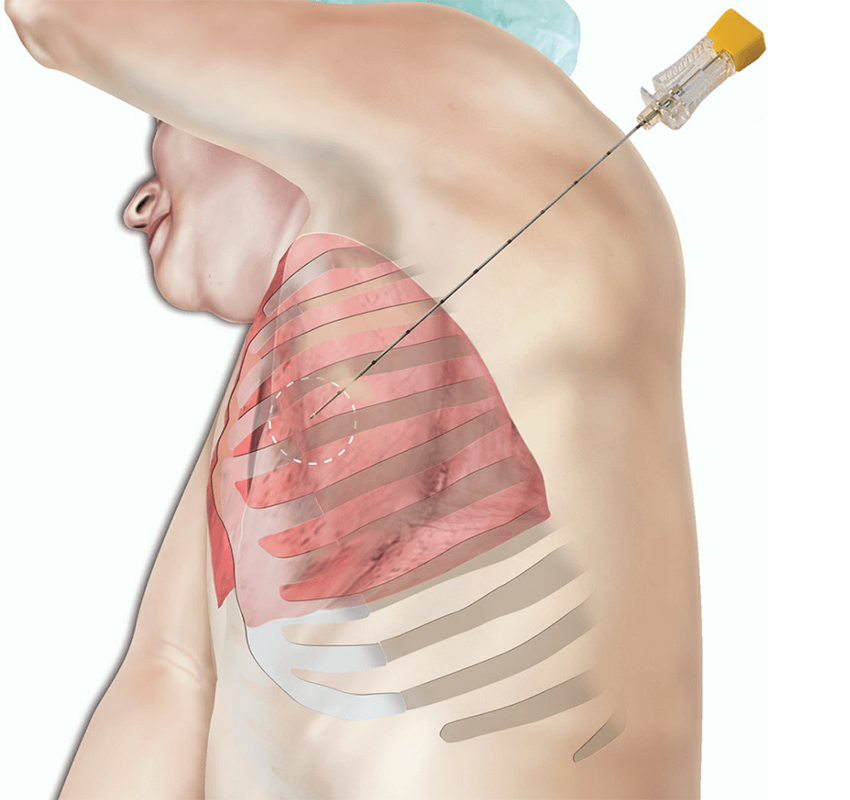
CTguided percutaneous biopsy
This is the most common method for lesions near the outer lung. The radiologist inserts a thin needle while watching on a CT scan. Because the needle travels through the chest wall, pneumothorax is the biggest worry, not seeding.
Bronchoscopic (EBUS) biopsy
Here a flexible scope with an ultrasound probe reaches the airway and samples nearby lymph nodes. The needle never leaves the airway, making tumor seeding virtually impossible.
Surgical (VATS) biopsy
Videoassisted thoracoscopic surgery is reserved for larger or hardertoreach tumors. It provides a bigger tissue sample but involves a small incision. Seeding is still exceedingly rare, but the procedure carries typical surgical risks.
Video suggestion
Embedding a short expert demonstration from a reputable medical site (e.g., ) would help visual learners grasp each technique.
Risks Of Other Biopsies
Skin biopsy
For skin lesions, a tiny punch or shave is taken. The seeding risk is essentially zero; skin heals quickly and any stray cells are usually cleared by the immune system.
Lymphnode biopsy
Whether done through a fineneedle aspiration or a small surgical excision, the odds of spreading cancer are minuscule. The main concern is accurate stagingnot seeding.
Comparative snapshot
- Skin biopsy 0% seeding.
- Lung biopsy ~0.010.05%.
- Lymphnode biopsy <0.01% (very rare).
Bottom line
If youve had a skin or lymphnode biopsy, you can breathe easythose procedures virtually never cause cancer to spread.
Common Patient Questions
Does cancer spread faster after biopsy?
Theres no solid evidence that a biopsy accelerates tumor growth. The biggest risk to your health is delaying treatment, not the biopsy itself.
If biopsy is negative, can it still be cancer?
Yes. No test is 100% perfect. A negative result could be due to sampling error, especially with small needles. Your doctor may recommend repeat imaging or a second biopsy if suspicion remains.
What is the most common complication of a lung biopsy?
Pneumothoraxair leaking into the space around the lungoccurs in about 1530% of percutaneous biopsies. Most cases are small and resolve with observation or a brief chest tube.
Are biopsies safe for cancer patients?
Overall, yes. The procedure is carefully planned to minimize risk, and the diagnostic information it provides is essential for tailoring therapy.
Do elderly patients face higher risk?
Older individuals may have a higher chance of pneumothorax or bleeding because of frailer lung tissue, but the seeding risk remains unchanged.
Minimizing Your Risk
Preprocedure checklist
- Review all imaging studies with your doctor.
- Ask about needle size and number of passes.
- Confirm the use of a coaxial sheath or tractsealant.
- Discuss any bloodthinning medications youre on.
During the procedure
- Ensure realtime imaging guidance (CT or EBUS).
- Ask the physician to limit the number of needle passes.
- Stay stillmovement can increase tissue trauma.
Postprocedure care
- Stay in the recovery area for at least 24hours for observation.
- Report any sudden chest pain or shortness of breath immediately.
- Follow up with a chest Xray (or CT) as instructed to check for pneumothorax.
Quickreference infographic idea
A 5 Steps to a Safer Lung Biopsy graphic would be perfect for sharing on social media and clinic waiting rooms.
Real Patient Stories
Story 1 Positive outcome, no seeding
Mark, a 58yearold former smoker, was nervous about a CTguided biopsy for a suspicious nodule. After the procedure, pathology confirmed earlystage adenocarcinoma. He began targeted therapy within two weeks and is now in remission. I was terrified of spreading the cancer, Mark says, but the doctors explained the risks, and the outcome was far better than the fear.
Story 2 Rare seeding case
Linda, 72, underwent a percutaneous biopsy that later revealed a tiny seed of tumor along the needle track. The surgical team removed the implanted nodule, and she continued her original treatment plan without further spread. It was scary at first, but catching it early saved me, she shares.
Lesson learned
Both stories underline that the huge majority of biopsies are uncomplicated, and even the rare seeding event can be detected and managed promptly.
Expert Insights Sources
Suggested expert voices
Invite a boardcertified pulmonologist (e.g., Dr. Emily Chen, 12years of CTguided biopsy experience) and a surgical oncologist (e.g., Dr. Raj Patel, specializing in thoracic oncology) to contribute quotes and bestpractice tips.
Credible sources to cite
- American Cancer Society Can a Biopsy Make Cancer Spread? (2025).
- Mayo Clinic research article on biopsy safety (2024).
- National Cancer Institute FAQs on biopsy risks.
- Peerreviewed case studies from Radiology and Journal of Thoracic Oncology.
How to reference
Throughout the article, insert superscript numbers linked to a reference list at the end (e.g., ).
Conclusion
Bottom line: a lung biopsy is a powerful diagnostic tool with an extremely low risk of spreading cancer. The most common complication is a harmless pneumothorax, not tumor seeding. By understanding the procedure, asking the right questions, and following pre and postprocedure care steps, you can move forward with confidence.
If youve been considering a biopsy or have already scheduled one, talk openly with your healthcare team about needle size, imaging guidance, and tracksealant use. Knowledge reduces anxiety, and a wellplanned biopsy can be the key that unlocks the most effective treatment plan.
Whats your experience with biopsies? Have you faced a similar worry? Share your story in the commentsyour voice could help someone else feel a little less alone.
For patients researching cancer treatment options and prognosis, resources on related topics may be helpful. For example, if you or a loved one is dealing with prostate cancer and wondering about long-term outcomes, see prostate cancer outlook for more information on prognosis and survivorship. If you are exploring treatment choices that include hormonal therapies, this overview of anti-androgens prostate cancer explains how those drugs work and potential side effects.
FAQs
Does a lung biopsy increase the chance of cancer spreading?
Studies show the risk of tumor seeding from a lung biopsy is about 0.01‑0.05 %, which is extremely low—roughly a few cases per million procedures.
What is tumor seeding and how often does it happen with lung biopsies?
Tumor seeding occurs when a few cancer cells are displaced along the needle track during a biopsy. It happens in about 1‑2 cases per million lung biopsies.
What are the most common complications of a lung biopsy?
The most frequent complication is pneumothorax (air in the chest cavity), occurring in 15‑30 % of percutaneous biopsies. Bleeding and infection are less common.
How can I reduce the risk of tumor seeding during a biopsy?
Ask your doctor about using a thin needle, limiting needle passes, employing a coaxial sheath, and applying a tract‑sealant. Real‑time imaging guidance also minimizes risk.
If a biopsy shows cancer, what are the next steps for treatment?
The result guides staging and helps select targeted therapies, surgery, radiation, or chemotherapy. Your oncology team will discuss the best personalized plan.