Short answer: TAVR isnt a good fit if youve had a recent heart attack, have very small or heavilycalcified access vessels, suffer from severe aorticroot disease, or your doctors estimate a life expectancy of less than one to two years. Its also usually skipped for younger, lowrisk patients, anyone with an active infection, or those who need a valve type that cant be delivered through a catheter.
Second short answer: If any of those red flags sound familiar, sit down with your heart team, bring this checklist, and talk openly about alternatives like surgical AVR (SAVR) or medical management. The goal is to find the safest path that matches your health goals and lifestyle.
Who Can Be a TAVR Candidate?
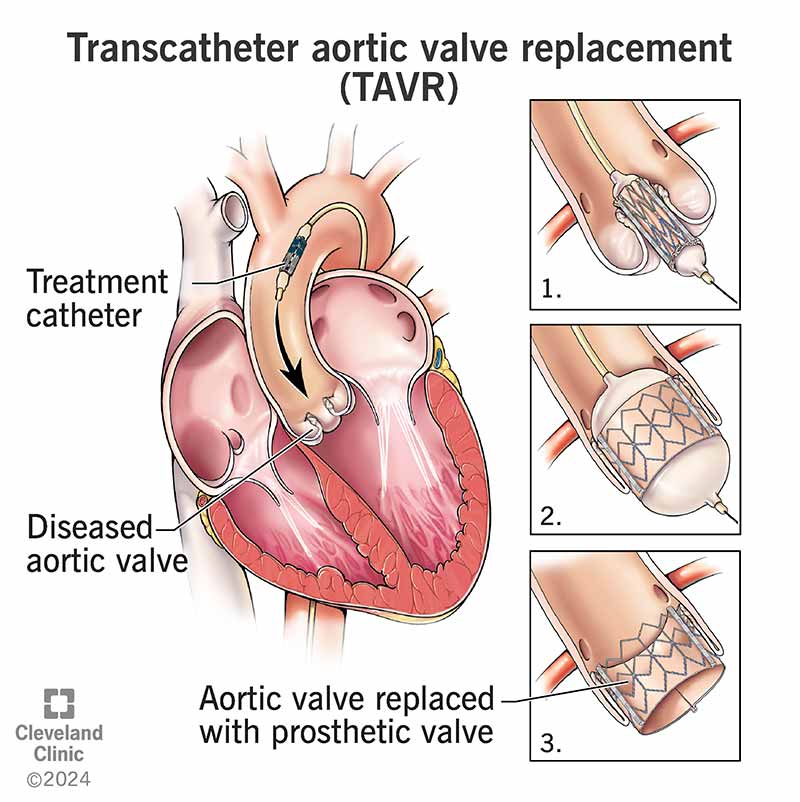
Transcatheter Aortic Valve Replacement (TAVR) is a minimally invasive way to replace a narrowed aortic valve without opening the chest. Its become popular because it usually means a shorter hospital stay and a quicker return to everyday activities. Most centers look for:
- Age65years (or younger if the surgical risk is high)
- Severe aortic stenosis thats causing symptoms such as shortness of breath, chest pain, or fainting
- Intermediatetohigh surgical risk measured by scores like STS or EuroSCORE
Dr. Lina Mendoza, a cardiothoracic surgeon at the Cleveland Clinic, notes that patient selection is as much an art as it is a scienceevery heart tells a slightly different story.
Core Reasons TAVR Is Not Recommended
Recent Heart Attack
A heart attack within the past 30days dramatically raises the risk of periprocedural myocardial injury. Studies show a 12% increase in mortality if TAVR is performed too soon after an MI. Most teams will wait at least a month, focusing first on stabilising the heart with medication.
Why the waiting period matters
- Healing of the heart muscle reduces the chance of further damage during rapid ventricular pacing.
- Bloodclotting dynamics normalize, lowering the risk of stroke.
- Patients often feel more energetic, making the procedure smoother.
Severe AorticRoot Disease
If the aortic root is aneurysmal (typically >5cm), dissected, or infected, a catheterdelivered valve cant anchor safely. In those cases, openheart surgery (SAVR) provides the best platform for repair.
Data snapshot
| Condition | Recommended Approach | 30Day Mortality |
|---|---|---|
| Aneurysm >5cm | SAVR with root replacement | 23% |
| Active infection (endocarditis) | Surgical debridement + valve | 57% |
Inadequate Vessel Size or Access
TAVR catheters travel through the femoral or iliac arteries. If those vessels are narrower than about 5mm, heavily calcified, or tortuous, the device cant pass safely. Attempting it could cause serious bleeding or limb loss.
Quick visual check
Imagine trying to push a garden hose through a narrow, rocky garden pathif the paths too tight, the hose will kink or burst. The same principle applies to catheters in tiny, calcified arteries.
Low Life Expectancy
When doctors project a life expectancy of less than 12yearsoften because of advanced cancer, severe COPD, or endstage renal diseaseTAVRs longterm benefits fade. The procedure itself carries a 23% earlymortality risk, which may outweigh any symptom relief.
Guideline cutoff
Most tertiary centers use a threshold of <2years, but the exact number can vary based on patient preferences and qualityoflife goals.
Younger, LowRisk Patients
If youre under 65years old and have a low surgical risk (STS score <3%), surgeons often favor SAVR because the mechanical or tissue valve placed surgically tends to last longer, and the durability data for TAVR in this group is still maturing.
Pros & Cons at a glance
| Option | Advantages | Disadvantages |
|---|---|---|
| TAVR | Shorter hospital stay, less pain | Potential for earlier valve degeneration in young patients |
| SAVR | Proven durability, easier future interventions | Openchest surgery, longer recovery |
Active Infection or Endocarditis
Placing a foreign object (the valve) in an infected environment can seed the device, leading to a 20%+ chance of prosthetic valve infectiona scenario thats notoriously hard to treat.
Severe LeftVentricular Dysfunction
If the leftventricles pumping ability is extremely low (ejection fraction <20%), the rapid pacing needed during TAVR can provoke dangerous drops in blood pressure. In such cases, surgeons may opt for a surgical approach that allows for simultaneous ventricular support.
Congenital Defects or Prior Valve Surgery
Patients with a bicuspid aortic valve thats heavily calcified, or who already have a mechanical valve elsewhere, often need a tailored surgical plan. Valveinvalve TAVR can work, but the anatomy must be carefully mapped.
Frequently Asked FollowUp Questions
What is the typical life expectancy after TAVR?
For patients with intermediate surgical risk, fiveyear survival hovers around 70%. Those with low risk do even better, approaching the outcomes of traditional surgery.
What are common side effects after TAVR surgery?
Most folks experience mild fatigue, a lowgrade fever, or temporary kidney irritation (AKI). Vascular complications like bleeding at the entry site occur in about 57% of cases but are usually manageable.
How does the risk of TAVR in the elderly compare to younger patients?
People 85years or older have a slightly higher chance of vascular complications, yet their 30day mortality is similar to that of 70yearolds when the procedure is properly selected.
What is the cost of a TAVR procedure in the U.S.?
Overall expenses usually fall between $40,000 and $50,000, covering hospital stay, the valve device, and physician fees. Insurance coverage varies, so its worth confirming details with your provider.
Is TAVR a major surgery?
Its minimally invasiveno sternum split, just a small puncture in the groin or chest. While not major in the traditional sense, its still a serious cardiac intervention that requires careful postprocedure monitoring.
Why do some patients feel fatigue after TAVR?
Recovery involves rebuilding strength after a period of limited activity. Anemia from blood loss, temporary deconditioning, and the hearts adjustment to the new valve can all contribute to lingering tiredness.
SAVR vs. TAVR: which is better for me?
The answer hinges on age, anatomy, surgical risk, and personal preference. Below is a quick decision matrix:
| Factor | SAVR | TAVR |
|---|---|---|
| Age<65&Low Risk | Preferred | Consider |
| Severe Calcified Vessels | Preferred | Not Ideal |
| High Surgical Risk | Risky | Ideal |
| Desire for Short Hospital Stay | Longer | Shorter |
Balancing Benefits & Risks A Practical Checklist
Print this out, bring it to your next appointment, and tick the boxes that apply to you.
| Yes Consider TAVR | No Explore Alternatives |
|---|---|
|
|
Remember, every heart is unique. Use this checklist as a conversation starter, not a final verdict.
RealWorld Cases & Expert Insights
| Case | Age | Reason TAVR Was Rejected | Outcome |
|---|---|---|---|
| A | 78 | Femoral artery 4mm too small | SAVR performed; uneventful recovery |
| B | 62 | Low surgical risk, age<65 | Chose SAVR per ; excellent valve durability at 5years |
| C | 84 | Life expectancy 9months (advanced cancer) | Opted for medical management; qualityoflife focus |
| D | 70 | Recent NSTEMI 2weeks ago | Delayed TAVR 6weeks; successful later |
Dr. Mendoza emphasizes, Clinical judgment, not just algorithms, decides the final path. Listening to the patients story is half the treatment.
Sources & Further Reading
All data points above are drawn from peerreviewed journals, reputable cardiology societies, and major heart centers. For deeper dives, you can explore the publications or the latest ACC/AHA guideline on valve disease. For information about recovery after valve procedures and tips on rehabilitation, see heart valve recovery.
Conclusion
TAVR has transformed the care of many people with severe aortic stenosis, but its far from a universal cureall. The biggest nogo signals are a recent heart attack, unsuitable vessel anatomy, serious aorticroot disease, limited life expectancy, and low surgical risk in younger patients. By weighing these factors against the benefitsshorter hospital stays, quicker return to daily lifeyou and your heart team can decide the safest, most effective route.
Take this checklist, discuss it openly with your cardiologist, and dont shy away from asking what if scenarios. Your heart deserves a plan thats both evidencebased and personally right for you.
FAQs
Who should generally avoid TAVR?
TAVR is usually not recommended for patients who had a recent heart attack (within 30 days), have very small or heavily calcified access vessels, severe aortic root disease, an active infection, or a life expectancy of less than 1-2 years.
Why is TAVR not advised soon after a heart attack?
Performing TAVR shortly after a heart attack raises the risk of myocardial injury and mortality. Waiting at least a month allows heart muscle healing, stabilizes blood clotting, and improves procedural safety.
What role does vessel size play in TAVR suitability?
TAVR catheters require access vessels at least about 5 mm in diameter without heavy calcification; smaller or tortuous vessels increase the risk of complications, making TAVR unsafe.
Why are younger, low-risk patients often advised against TAVR?
For patients under 65 with low surgical risk, surgical aortic valve replacement (SAVR) is preferred due to better valve durability and more established long-term outcomes compared to TAVR.
Can TAVR be performed if there is an active infection?
No, active infection, especially endocarditis, is a contraindication because inserting a valve prosthesis in an infected environment risks serious prosthetic valve infection.