Got a weirdly high bloodpressure reading after you roll out of bed? Thats supine hypertension a condition where your numbers shoot up while youre lying flat. It usually stems from the way your nervous system, heart, or bloodvessel tone are out of sync, and spotting the root cause early can keep you from the headaches and organ stress that follow.
Understanding why this happens, what it feels like, and how to tame it isnt just medical trivia; its the first step toward feeling safe again at night. Lets break it down together, no jargon, just a friendly chat.
Understanding Supine Hypertension
What is supine hypertension?
Supine hypertension is defined as a bloodpressure reading of 140/90mmHg or higher after youve been lying down for 510minutes. Its the opposite of orthostatic hypotension, which drops when you stand. In other words, your bodys lyingdown alarm is stuck on high.
How is it measured?
First, sit quietly for a few minutes, then lie flat on a firm surface. Keep the cuff at heart level and take three readings, spacing them a minute apart. Average those numbers and youve got your supine value. For home monitoring, the same process works just make sure the cuff isnt too tight and youre breathing normally.
Blood Pressure Supine vs Sitting
| Position | Typical Systolic (mmHg) | Typical Diastolic (mmHg) |
|---|---|---|
| Supine | 130150 | 8095 |
| Sitting | 115130 | 7085 |
Who gets it?
Anyone can develop supine hypertension, but its especially common in people with autonomic nervous system disorders think Parkinsons disease, multiple system atrophy (MSA), or pure autonomic failure. Older adults also see it more often because their bloodvessel elasticity declines with age.
Primary Causes Explained
Autonomic nervous system dysfunction
When the baroreceptors (the pressuresensing nerves in the neck and chest) cant talk properly to the brain, the sympathetic nervous system may overreact, tightening vessels even when youre flat. This malfunction is a big driver of supine hypertension causes in neurogenic patients.
Excessive cardiac output
Some folks simply pump more blood when they lie down the hearts stroke volume rises because the veins return blood more easily. If the vessels dont relax enough, that extra flow translates into higher pressure.
High vascular resistance
Even with normal heart output, the arteries can stay constricted. Hormones like endothelin or an overactive reninangiotensin system keep the tone high, especially after a salty dinner or a latenight drink.
Medications that raise supine BP
- Midodrine a shortacting 1agonist often used for orthostatic hypotension, but it can backfire at night.
- Droxidopa similar effect, especially if taken close to bedtime.
- Decongestants (pseudoephedrine)
- Selective serotonin reuptake inhibitors (SSRIs) and SNRIs
- Corticosteroids
Knowing this helps you and your doctor adjust timing or dosage.
Coexisting conditions
| Condition | Why it contributes | Typical scenario |
|---|---|---|
| Parkinsons disease | Degeneration of autonomic nuclei | Morning headaches, low standing BP, high supine BP |
| Multiple system atrophy | Impaired baroreflex | Fluctuating pressures throughout the night |
| Chronic kidney disease | Fluid overload and RAAS activation | Consistently high supine numbers |
| Obstructive sleep apnea | Intermittent hypoxia spikes sympathetic tone | Sudden spikes during REM sleep |
Lifestyle and environmental triggers
Its not all about disease. A heavy, salty meal before bed, a nightcap of alcohol, or even a snug blanket that restricts venous return can push your pressure higher. Small changes like cutting the latenight chips or sleeping with the head of the bed elevated often make a noticeable difference.
Symptoms and Risks
Typical symptoms
Most people notice a pounding headache when they sit up, occasional dizziness, or blurry vision. Some report a feeling of pressure in the chest that eases once they stand. These are the classic supine hypertension symptoms.
When it becomes dangerous
If your nighttime readings consistently top 180/110mmHg, youre walking a line toward stroke, heartfailure remodeling, or kidney injury. The risk isnt just theoretical studies have linked sustained supine spikes with accelerated organ damage, especially in older adults.
Overlap with orthostatic hypotension
It sounds paradoxical, but many patients swing between low standing pressure and high lyingdown pressure. This SHOH combo can be confusing, which is why logging both positions (see the checklist later) is crucial.
Diagnosis and Evaluation
Clinical workup checklist
- Review every medication, including overthecounter cold remedies.
- Perform a tilttable test to gauge baroreflex sensitivity.
- Order labs: electrolytes, plasma renin activity, aldosterone, cortisol.
- Record supine and sitting pressures on three separate mornings.
Imaging and referrals
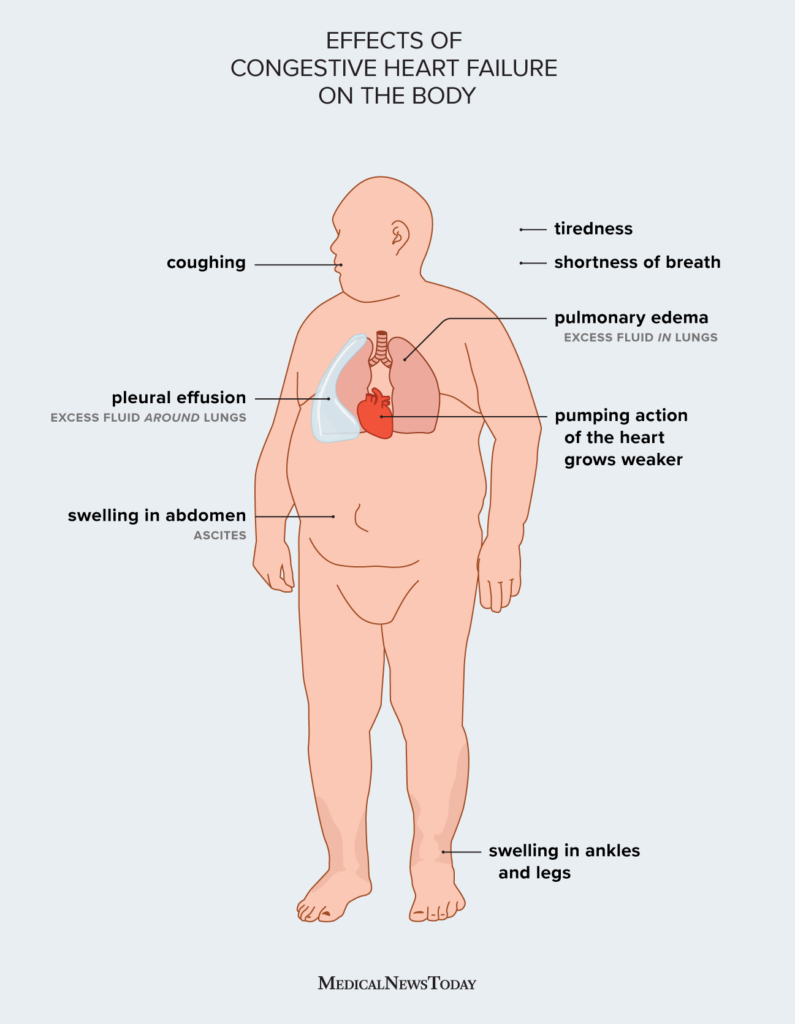
A cardiac echocardiogram can reveal whether an inflated cardiac output is part of the picture. If neurogenic causes are suspected, a neurologist familiar with autonomic disorders should weigh in. In complex cases, a multidisciplinary clinic (cardiology + neurology) often yields the best plan. For patients with heart-related fluid issues contributing to nighttime pressure, consider evaluating for heart failure edema as part of the workup.
Treatment Options Overview
Nonpharmacologic first line
Start simple: raise the head of your bed 3045 degrees with pillows or an adjustable base. This slight tilt helps gravity pull blood away from the heart, lowering the pressure. Pair that with a lowsodium dinner (under 1,500mg) and avoid caffeine after 5p.m.
Pharmacologic options
| Drug | Mechanism | When to use | Main risk |
|---|---|---|---|
| Shortacting nifedipine | Calciumchannel blocker | Isolated supine spikes | Reflex tachycardia |
| Lowdose captopril | ACE inhibitor | Renalrelated hypertension | Cough, hyperkalaemia |
| Clonidine (bedtime, low dose) | Central 2agonist | Autonomic SH | Sedation, dry mouth |
| Midodrine (shortacting) | Peripheral 1agonist | Neurogenic SH (with caution) | Can worsen supine hypertension monitor closely |
Note the nuance: midodrine may be useful for orthostatic lows, but youll need to time the dose so it wears off before bedtime.
Managing SH in Parkinsons disease
If youve got Parkinsons, the interplay between dopaminergic meds and blood pressure becomes a dance. Often, adjusting levodopa timing (taking it earlier in the day) and adding a lowdose bedtime clonidine can smooth out the peaks and valleys.
Balancing benefits and risks
Every treatment carries a tradeoff. The goal is to keep supine BP under control without causing severe orthostatic hypotension. Thats why many clinicians prefer a start low, go slow approach, monitoring both positions each week.
Practical Checklist Tools
Morning BP QuickCheck
Print a simple table and fill it out each morning:
| Date | Supine (mmHg) | Sitting (mmHg) | Symptoms? | Notes |
|---|---|---|---|---|
| 20250801 |
Medication audit worksheet
List each medicine, its dose, the time you take it, and whether youve noticed a BP change. This helps you and your doctor pinpoint culprits like midodrine at 8pm = supine 160/95.
Trusted resources
For deeper dives, check out the American Autonomic Society guidelines, recent AHA hypertension statements, and patientshared stories on patient forums. Realworld anecdotes often illuminate what the textbooks cant.
Key Takeaways Summary
Supine hypertension isnt a mysterious overnight curse its usually a signaltonoise problem in your bodys pressureregulating system. By recognizing the common triggers (autonomic dysfunction, certain meds, lifestyle factors) and tracking both supine and sitting readings, you empower yourself to make informed choices. Simple steps like elevating the head of the bed, watching salt intake, and reviewing medication timing often bring the numbers down without heavy pills. When drugs are needed, a lowdose, shortacting regimen monitored by a knowledgeable clinician can keep the highs in check while protecting you from orthostatic lows.
Now that youve got the big picture, why not try the quickcheck table tonight? And if youve experimented with any tricks headup pillows, diet tweaks, or timing tweaks share your story in the comments. Were all learning together, and every tip could be the one that helps someone else finally get a peaceful nights sleep.
FAQs
What are the most common causes of supine hypertension?
The condition usually stems from autonomic nervous system dysfunction, certain blood‑pressure‑raising medications, excess cardiac output when lying flat, high vascular resistance, and lifestyle factors such as a high‑salt diet or alcohol before bed.
How can I tell if my medication is raising my supine blood pressure?
Track your supine and sitting readings each morning and note the time you take each drug. If a spike consistently follows a particular medication (e.g., midodrine taken at night), that drug is likely contributing.
What lifestyle changes can lower supine hypertension?
Try sleeping with the head of the bed elevated 30–45°, limit sodium to <1,500 mg after dinner, avoid caffeine and alcohol late in the day, and keep a low‑salt, balanced diet.
Is it safe to use blood‑pressure medication at night for supine hypertension?
Short‑acting agents such as low‑dose nifedipine or bedtime clonidine can be effective, but they must be prescribed and monitored closely to avoid worsening orthostatic hypotension.
When should I see a doctor about supine hypertension?
Schedule an appointment if your nighttime readings regularly exceed 180/110 mm Hg, if you experience headaches or blurry vision upon standing, or if you have any underlying conditions like Parkinson’s disease or chronic kidney disease.