Got that nagging knee ache or ankle throb and wonder if a tiny piece of bone is playing hideandseek inside your joint? An osteochondritis dissecans MRI can spot that fragment with roughly 92% sensitivity and 90% specificity, giving you a crystalclear picture of whats really going on. In the next few minutes well walk through why MRI is the goldstandard, decode the grading numbers, explore when surgery becomes an option, and show you how a healed lesion looks on followup scans all in plain, friendly language you can actually use.
Why MRI Matters
When doctors first suspect osteochondritis dissecans (OCD), they often start with an Xray. Xrays are great for spotting obvious bone defects, but theyre as good at judging stability as a selfie is at measuring your height. Stabilitya key factor that determines whether you can stay on the sidelines or need an operationrequires seeing the cartilage surface, the subchondral bone, and any fluid that may be creeping into the lesion. Thats where MRI shines.
Magnetic resonance imaging gives you threedimensional detail without radiation, letting radiologists evaluate:
- Whether the fragment is still attached or has become loose.
- How much swelling (bone marrow edema) surrounds the spot.
- The condition of the overlying cartilage.
According to , MRIs ability to differentiate a stable from an unstable lesion is the reason its the goto test for both knee and talus OCD.
MRI Grading System
When you stare at the MRI images, youll see a series of grades that look a bit like school report cards. Most radiologists use a 04 scale, sometimes called the Hefti or Kellgren grading system. Heres a quick rundown:
| Grade | What It Means |
|---|---|
| 0 | Normal no lesion visible. |
| 1 | Small area of signal change; fragment is stable. |
| 2 | Fragment still attached, but theres a fluid rim indicating early instability. |
| 3 | Clear separation or highsignal fluid line fragment is unstable. |
| 4 | Detached fragment, possibly displaced into the joint. |
For the ankles talus (the OCD talus), the grading is similar but often emphasizes the dome region of the bone. The principles stay the samehigher grade equals higher risk of detachment. Understanding these grades can help patients distinguish between different stages of joint inflammation similar to spine inflammation.
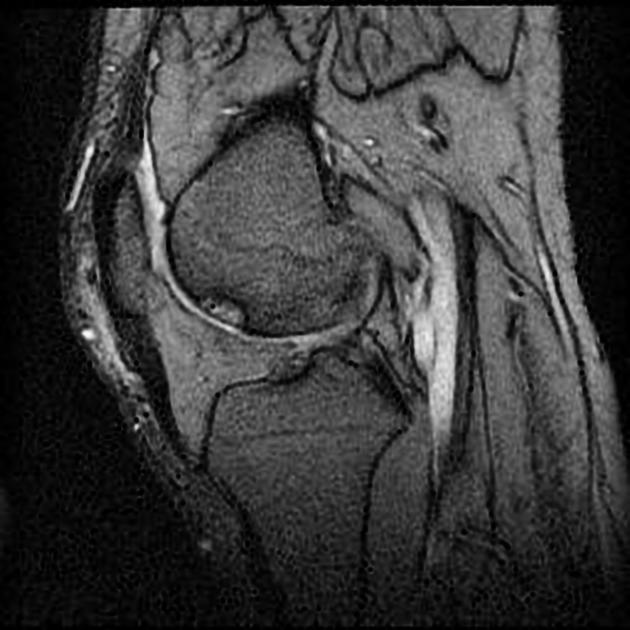
Reading the Scan
Imagine youre a detective with a magnifying glass. The typical lookfirst checklist goes something like this:
- Coronal T2fatsat (FS): Start here to locate the lesion and gauge its size.
- Sagittal protondensity (PD): This slice shows the cartilage capcrucial for judging stability.
- Axial T1: Gives you a sense of the subchondral bones internal signal.
Key signs of instability include a bright fluid rim surrounding the fragment, a displaced piece of bone, or secondary cysts forming around it. If you spot these, the odds are youre looking at a grade3 or4 lesion, and the treatment conversation will shift toward surgical options.
Heres a quick anecdote: I once met a 15yearold soccer enthusiast whose MRI showed a shiny, fluidfilled cleftclassic grade3. His doctor explained that staying on the field could worsen the fragment, so they opted for arthroscopic fixation. Six months later, his followup MRI showed the fragment glued back, and he was back scoring goals.
Deciding on Treatment
Now comes the part most of us worry about: Do I need surgery? The answer hinges on three thingsgrade, symptoms, and time.
- Stable, lowgrade lesions (02): Usually respond well to activity modification, a brief period of casting or bracing, and targeted physical therapy such as osteoporosis physical therapy. Many patients return to sport within 36months.
- Unstable, highgrade lesions (34): These often need surgical fixation, microfracture, or osteochondral autograft transplantation. Studies show success rates of 7085% for returning to preinjury activity after proper fixation.According to a 2020 cohort study, early surgery (within 3months of diagnosis) improves healing odds.
- Persistent pain after conservative care: If symptoms linger beyond 36months despite rest and rehab, a repeat MRI can reveal whether the lesion has progressed, prompting a timely surgical referral.
After surgery, a followup MRI at 36months helps confirm healing. A healed OCD MRI typically shows recontoured cartilage, disappearance of the fluid rim, and reduced marrow edema. Some residual signal may linger, but its usually benign scar tissue.
Joint Specific Insights
While the knee gets most of the spotlight, OCD can pop up in the ankle (talus) and even the elbow (capitellum). Each joint has its quirks.
- Knee OCD: Frequently appears on the medial femoral condyle. Look for the classic Cshaped lesion on coronal images. Pitfall: a thin cartilage fissure can masquerade as a fragmentalways confirm with multiple planes.
- Talus OCD: The lesion usually sits on the dome of the talus. Because the ankle bears weight from all directions, even a small grade2 lesion can cause deep ankle pain and swelling. Early detection often saves the need for fusion surgery later on.
- Elbow OCD: Common in young baseball pitchers. MRI shows a lesion in the capitellum, often with a tiny fluid crescent. Prompt rest and rehab can prevent progression to a grade3 lesion that would otherwise demand surgery.
Practical Takeaway Checklist
Feel free to print this out or save it on your phonethinking of it as a quick cheat sheet before your next orthopaedic appointment.
- Ask your doctor why an MRI is recommended (stability assessment).
- Know your lesions grade: 01=stable, 24=potentially unstable.
- Check for fluid rims, subchondral cysts, or displaced fragments on the images.
- If you have a grade34 lesion, discuss surgical options earlydelaying can worsen outcomes.
- Plan a followup MRI 36months after treatment to verify healing.
- Stay active, but respect the rehab timeline; overdoing it can reignite the injury.
Remember, the goal isnt just to get a label on a scan; its to guide you back to the activities you lovewhether thats kicking a soccer ball, dancing at a wedding, or simply walking your dog without wincing.
Conclusion
In a nutshell, an osteochondritis dissecans MRI gives you the detailed map you need to understand whether your joint lesion is stable or ready to cause trouble. Knowing the grading, spotting the key signs of instability, and aligning those findings with appropriate treatment (conservative or surgical) empowers you to make informed decisions and keep moving forward. If you or someone you know is navigating an OCD diagnosis, bring this checklist to the orthopaedist, ask about the specific grade, and stay curious about your progress. Got questions or personal stories to share? Drop a comment belowwere all in this together, and Im happy to help you figure out the next step.
FAQs
What does an osteochondritis dissecans MRI reveal?
An osteochondritis dissecans MRI visualizes the cartilage surface, sub‑chondral bone, and any surrounding fluid, allowing doctors to assess fragment stability, bone marrow edema, and cartilage health.
How are OCD lesions graded on MRI?
Radiologists usually use a 0‑4 scale (Hefti/Kellgren). Grade 0 is normal, 1‑2 are stable lesions, while grades 3‑4 indicate increasing instability or a detached fragment.
When is surgery recommended for OCD based on MRI findings?
Surgery is typically advised for unstable, high‑grade lesions (grade 3‑4) or when symptoms persist after 3‑6 months of conservative care, especially if the MRI shows a fluid rim or displaced fragment.
Can a follow‑up MRI confirm healing after treatment?
Yes. A healed OCD MRI usually shows a re‑contoured cartilage surface, disappearance of the fluid rim, reduced marrow edema, and no evidence of fragment displacement.
Is an MRI necessary for every suspected OCD case?
While X‑rays can detect obvious bone defects, MRI is the gold‑standard for evaluating stability and cartilage condition, making it essential for accurate diagnosis and treatment planning.