Looking for the right psoriatic arthritis drug that eases your joint pain and keeps your skin clear? Short answer: start with NSAIDs for occasional flareups, move to conventional DMARDs like methotrexate for diseasemodifying control, and consider biologics or JAK inhibitors when the disease is moderatetosevere. Each step balances how well the drug works with its safety profile.
Choosing a medication isnt just about numbers on a label; its about fitting a treatment into your life, your health history, and even your budget. Below youll find a friendly roadmap that covers the most commonly prescribed drugs, how theyre tested, realworld experiences, and practical tips you can use today.
Quick Summary Table
Top8Psoriatic Arthritis Drugs at a Glance
| Drug Class | Brand Name | Typical Use | Key Benefit | Major Safety Note |
|---|---|---|---|---|
| NSAID | Ibuprofen, Naproxen | Mild flare pain | Fast pain relief | Stomach irritation, blood pressure |
| Conventional DMARD | Methotrexate | Earlymoderate disease | Slows joint damage | Liver monitoring required |
| TNF Inhibitor | Adalimumab (Humira) | Moderatesevere joint & skin | High efficacy, quick skin response | TB reactivation risk |
| IL12/23 Inhibitor | Ustekinumab (Stelara) | Skindominant disease | Long dosing interval (12weeks) | Infection risk, rare malignancy |
| IL17 Inhibitor | Secukinumab (Cosentyx) | Joint & severe skin involvement | Strong joint protection | Candidiasis, neutropenia |
| JAK Inhibitor | Upadacitinib (Rinvoq) | Oral option after biologic failure | Convenient pill, rapid relief | Thromboembolic risk |
| PDE4 Inhibitor | Apremilast (Otezla) | Mildmoderate disease | No injections, low infection risk | GI upset, weight loss |
| Glucocorticoid | Prednisone | Shortterm flare control | Powerful antiinflammatory | Bone loss, glucose rise |
How Drugs Work
What Is a Biologic and Why Does It Matter?
Biologics are engineered proteins that target specific immune signalsmost often tumor necrosis factoralpha (TNF). By blocking this messenger, drugs like etanercept, adalimumab, and infliximab calm the fire that damages joints and skin. , patients on TNF inhibitors often experience a 5060% improvement in joint pain within weeks.
NonBiologic DMARDs The Backbone of Therapy
Conventional diseasemodifying antirheumatic drugs (DMARDs) such as methotrexate and leflunomide work by broadly suppressing immune cell proliferation. They arent as targeted as biologics, but theyre proven, inexpensive, and have decades of safety data behind them. The tradeoff is slower onsetusually a few months before you notice a real difference.
JAK Inhibitors The New Oral Option
Janus kinase (JAK) inhibitors, like upadacitinib, act inside immune cells to stop the cascade that fuels inflammation. The appeal? A oncedaily pill that can be just as effective as an injection. However, they carry a warning about rare blood clot events, so regular lab checks are a must.
Medication Categories
When to Choose Each Class
- NSAIDs Best for occasional flareups when you need quick pain relief without changing your longterm regimen.
- Conventional DMARDs Ideal for earlytomoderate disease, especially when skin symptoms are mild.
- TNF Inhibitors Firstline biologic for most patients with moderatetosevere joint and skin involvement.
- IL12/23 or IL17 Inhibitors Consider when skin disease dominates or if youve had a suboptimal response to a TNF blocker.
- JAK Inhibitors Good oral alternative after biologics, especially for patients who dislike injections.
- PDE4 Inhibitors Lower infection risk, suitable for people with mild disease who prefer a pill.
What Are the 5 Types of Psoriatic Arthritis?
Psoriatic arthritis isnt onesizefitsall. Clinicians usually describe five patterns:
- Symmetric polyarthritis mirrors rheumatoid arthritis.
- Asymmetric oligoarthritis a few joints on one side.
- Distal interphalangeal (DIP) predominant affects the fingertips.
- Spondylitis involves the spine and sacroiliac joints.
- Arthritis mutilans severe, destructive form (rare).
Knowing your pattern helps the rheumatologist pick the most effective psoriatic arthritis drug for you.
Choosing the Right
How Does a Rheumatologist Test for Psoriatic Arthritis?
A thorough exam starts with a medical history and a look at your skin. The doctor will then assess joint swelling, range of motion, and may order imagingXrays, ultrasound, or MRIto spot hidden erosions. Blood tests (CRP, ESR) can flag inflammation, even though theres no single psoriasis blood marker. , a combined clinicalradiographic approach yields the most accurate diagnosis.
What Is the Safest Drug for Psoriatic Arthritis?
Safest depends on your personal health story. Generally, nonbiologic DMARDs have a long safety track record but need liver monitoring. Biologics have excellent efficacy but require screening for latent tuberculosis and vigilance for infections. For patients with a history of recurrent infections, apremilast (a PDE4 inhibitor) is often considered the safest oral choice because it doesnt suppress the immune system as aggressively.
Personal Factors That Influence Choice
- Age & comorbidities Liver disease, heart disease, or pregnancy limit certain drugs.
- Injection vs. oral preference Some people love a weekly shot; others prefer a pill.
- Insurance coverage Biologics can be pricey; manufacturer copay cards may help.
- Lifestyle Travel, work schedules, and family planning all matter.
DecisionTree Snapshot
1 Mild symptoms NSAIDs + topical steroids
2 Persistent joint pain Methotrexate or leflunomide
3 Moderatesevere disease TNF inhibitor (adalimumab)
4 Skindominant or biologicfailed IL17 inhibitor (secukinumab) or JAK inhibitor (upadacitinib)
Benefits vs Risks
Common Side Effects by Class
- NSAIDs: stomach upset, higher blood pressure.
- DMARDs: liver enzyme elevation, nausea.
- TNF inhibitors: risk of TB, fungal infections.
- IL17 blockers: mouth thrush, neutropenia.
- JAK inhibitors: blood clots, elevated cholesterol.
LongTerm Safety Data
Postmarketing surveillance over the past decade shows that biologics have not increased overall cancer rates compared with the general population, though rare cases of lymphoma have been reported. continues to monitor safety signals, and most drugs retain a favorable riskbenefit ratio when used under specialist care.
Benefit vs Risk Scores
| Drug Class | Benefit Score (05) | Risk Score (05) |
|---|---|---|
| NSAIDs | 2 | 2 |
| Conventional DMARDs | 3 | 3 |
| TNF Inhibitors | 5 | 3 |
| IL17 Inhibitors | 5 | 2 |
| JAK Inhibitors | 5 | 4 |
Real World Questions
I Cured My Psoriatic Arthritis Is It Possible?
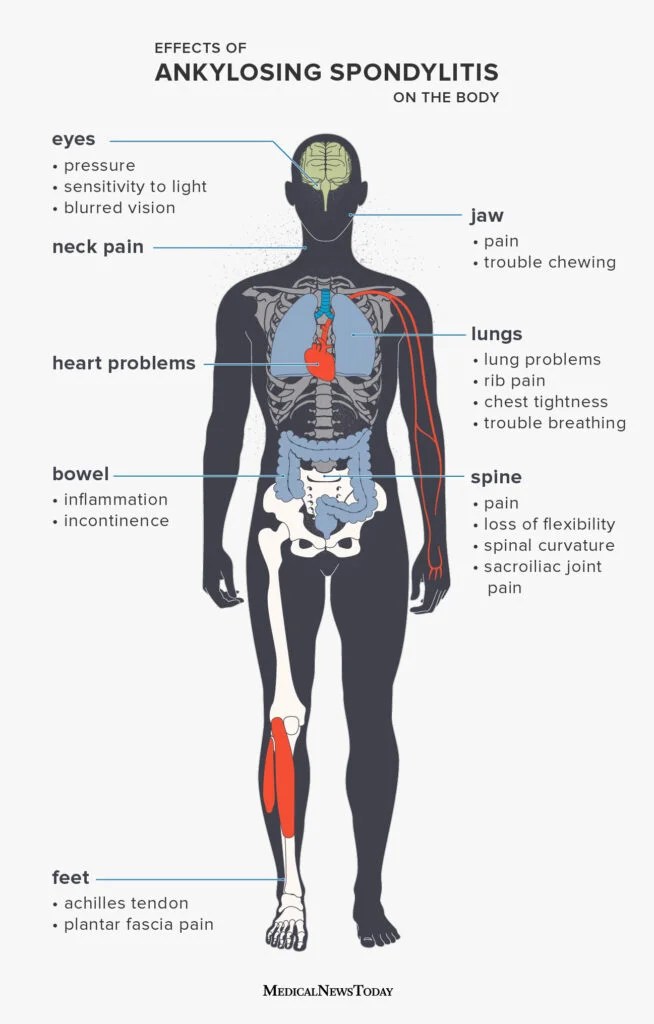
Cure is a strong word. What many patients experience is remissionthe disease is controlled so well that symptoms disappear and joint damage halts. A 2022 registry study found that roughly 20% of patients on biologics achieve sustained remission for at least one year. So, while the word cure feels hopeful, its more accurate to talk about longterm remission. For patients with spine involvement, tracking ankylosing spondylitis remission criteria can be helpful when discussing goals with your rheumatologist.
What Is the Best Pain Medication for Psoriatic Arthritis?
For quick pain relief, NSAIDs are usually firstline. If inflammation is high, a short course of lowdose prednisone can bridge the gap until DMARDs or biologics kick in. However, chronic reliance on opioids is discouraged because they dont address the underlying inflammation and carry addiction risks.
Can I Switch Between Drugs Safely?
Yes, but it requires a washout period to let the previous drug clear from your systemtypically a few weeks for most biologics, longer for some TNF inhibitors. Your rheumatologist will also check for antibodies that might reduce the new drugs effectiveness.
Do Lifestyle Changes Influence Medication Needs?
Absolutely. Maintaining a healthy weight reduces joint stress, while quitting smoking improves biologic response. Regular lowimpact exercise (swimming, cycling) can keep joints supple and may allow a lower medication dose.
Practical HowTo Guides
How to SelfInject a Biologic (StepbyStep)
- Wash your hands and gather the prefilled syringe.
- Choose an injection siteabdomen or thigh, rotating each time.
- Clean the skin with an alcohol swab.
- Pinch the skin, insert the needle at a 90 angle.
- Press the plunger slowly, wait the recommended time (usually 510seconds).
- Remove the needle, apply gentle pressure, and dispose of safely.
Monitoring Schedule: Labs & Appointments
Most doctors recommend baseline labs before starting a DMARD or biologic, then repeat tests at 46 weeks, 3 months, and every 612 months thereafter. Keep track of any new symptomsespecially fever, persistent cough, or unexplained rashesas these could signal infection.
Insurance & Financial Assistance Tips
Many pharmaceutical companies offer copayassist cards for biologics. Additionally, patientsupport programs like can provide coupon codes, free medication samples, or help navigate priorauthorization paperwork.
Bottom Line Takeaways
- Start simple: NSAIDs for occasional flareups.
- Escalate wisely: DMARDs for diseasemodifying control, biologics or JAK inhibitors for moderatetosevere disease.
- Safety matters: Screen for TB, monitor liver function, and discuss pregnancy plans.
- Partner with your rheumatologist: Regular labs, imaging, and open conversation keep your treatment on track.
Conclusion
Choosing the right psoriatic arthritis drug is a deeply personal decision that should blend clinical evidence with your everyday reality. By understanding how each medication works, weighing its benefits against its risks, and staying proactive with monitoring, you can move from a place of uncertainty to confident, informed care. If any part of this guide sparked a questionor you have a story about finding the perfect medicationshare it in the comments. Were all in this together, and your experience could guide someone else toward the relief they deserve.
FAQs
What is the first-line drug for psoriatic arthritis?
NSAIDs are generally used first for mild flare-ups, while conventional DMARDs like methotrexate are preferred for early to moderate disease; biologics such as TNF‑α inhibitors are first-line for moderate-to-severe cases.
How do biologic drugs work in psoriatic arthritis?
Biologics target specific immune molecules, most often tumor necrosis factor-alpha (TNF‑α), to reduce inflammation and prevent joint and skin damage.
Are oral options available besides injections for psoriatic arthritis?
Yes, JAK inhibitors (e.g., upadacitinib) and PDE‑4 inhibitors (e.g., apremilast) provide effective oral alternatives especially after biologic therapy or for mild disease.
What are the main risks associated with psoriatic arthritis drugs?
Risks vary by drug class: NSAIDs can cause stomach irritation and raise blood pressure; DMARDs require liver monitoring; biologics may increase infection risk including tuberculosis; JAK inhibitors carry blood clot risks.
Can psoriatic arthritis be cured with medication?
Psoriatic arthritis cannot be cured, but many patients achieve long-term remission with appropriate medications, effectively controlling symptoms and halting joint damage.