Did you know that a false joint can develop when bone that should have fused stays loose, causing pain that feels like a stubborn ache you just cant shake off? In plain English, pseudarthrosis (or pseudoarthrosis) is the medical term for that unwanted joint a spot where bone failed to merge into a solid piece after a fracture or spinal surgery.
Understanding this definition isnt just trivia; its the first step to spotting warning signs early, deciding whether you need a second opinion, and choosing the right treatment path. Below well walk through everything you need to know from why it happens to how doctors diagnose it, the treatment options on the table, and the everyday impact on life and work.
Clinical Overview
What Is Pseudarthrosis?
At its core, pseudarthrosis means false joint. After a bone break or a spinal fusion, the bodys natural healing process should create new bone that bridges the gap. When that bridge never forms, a fibrous tissue fills the space, acting like a shaky joint. This can happen in long bones (like the femur) or in the spine especially after lumbar fusion procedures.
Types of Pseudarthrosis
Doctors break it down into a few categories:
- Fibrous mostly soft tissue, very mobile.
- Bony some bone forms, but not enough for stability.
- Hypertrophic the body tries hard to heal, creating excess bone growth that still doesnt bridge.
- Atrophic poor healing response, little new bone at all.
How It Differs From NonUnion
While nonunion and pseudarthrosis are often used interchangeably, the subtle difference lies in the presence of that false joint. In a nonunion the bone simply hasnt united; in pseudarthrosis theres an actual pseudojoint that can move, causing more pronounced symptoms.
QuickReference Table
| Aspect | Pseudarthrosis | NonUnion |
|---|---|---|
| Definition | False joint formation | Absence of bone union |
| Typical Imaging | Gap with motion on flexextension Xray | Persistent radiolucent gap |
| Symptoms | Instability, sharp pain, audible clicking | Generalized dull pain |
Why It Happens
PostSurgical Failure (Lumbar Fusion)
Spinal surgeons aim for solid fusion, especially at the L5S1 level, but factors like smoking, diabetes, or inadequate bone graft can derail the process. A 2023 study of 1,200 lumbar fusions found that patients who continued smoking were 3.5 times more likely to develop pseudarthrosis at L5S1.
Traumatic NonUnion
Highenergy fractures (think car accidents) can damage the blood supply needed for bone healing. When the bodys repair crew cant get to the site, a false joint may develop. The same risk shoots up if youve got osteoporosis or chronic steroids in your system.
Biological Factors
Poor vascularity, infection, or even a genetic tendency toward weak bone remodeling can be the silent culprits. Researchers at the National Center for Biotechnology Information note that low levels of vitamin D and calcium are linked to higher pseudarthrosis rates.
RiskFactor Checklist
- Smoking within 6 weeks before/after surgery
- Uncontrolled diabetes or high blood sugar
- Obesity (BMI>30)
- Use of chronic steroids or immunosuppressants
- Insufficient bone graft material
Spotting the Problem
General Pseudarthrosis Symptoms
Typical clues include persistent, sharp pain that worsens with movement, a feeling that the affected area is wiggly, and sometimes an audible clicking or grinding. Unlike normal postop soreness, the pain doesnt improve with time and may even intensify after months.
LumbarSpine Specific Signs (L5S1)
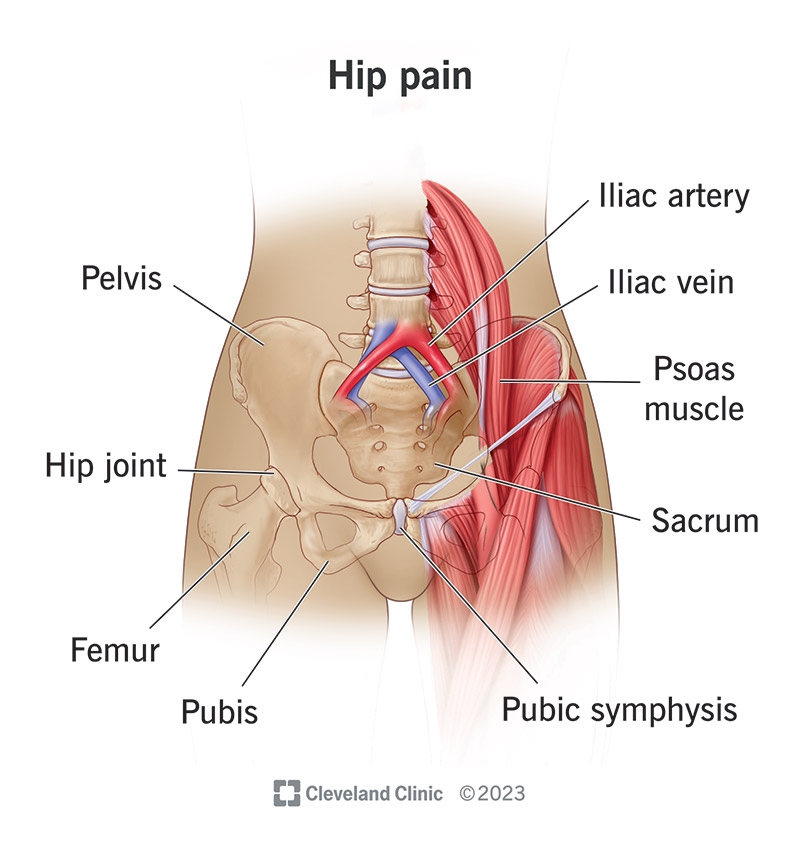
If the false joint is in the lumbar spine, expect lowerback ache that radiates into the buttocks or thighs, often accompanied by stiffness when you try to bend forward. Many patients also notice an unsettling sensation of giving way when lifting objects.
RedFlag Signs That Need Urgent Care
Sudden neurological deficits (numbness, weakness in the legs), loss of bladder or bowel control, or a rapid increase in pain after a minor fall are warning lights that call for immediate medical attention.
SymptomComparison Chart
| Condition | Typical Pain | Movement Effect | Additional Clues |
|---|---|---|---|
| Normal PostOp Recovery | Dull, improves over weeks | Gradual increase in flexibility | Lowgrade swelling only |
| Pseudarthrosis (Lumbar) | Sharp, localized, persistent | Instability, clicking on flexion | Radiating leg pain, giving way |
Diagnosis Steps
Imaging Toolbox
Radiographs (Xrays) are the first glance, but a CT scan gives the clearest picture of bony continuity. MRI can help rule out infection or disc issues, while flexionextension Xrays show the actual motion at the suspected joint.
Radiographic Criteria
Most surgeons look for an absence of bridging bone across the fusion site after 612 months, plus signs of hardware loosening (screw halo) on CT. The presence of a radiolucent gap that changes width with movement is a classic hallmark.
Laboratory Workup
Blood tests for inflammatory markers (CRP, ESR) and metabolic panels (calcium, vitamin D) help exclude infection or metabolic bone disease that could be masquerading as pseudarthrosis.
Diagnostic Flowchart
| Step | What to Do | Why |
|---|---|---|
| 1. Clinical Evaluation | History + Physical Exam | Identify pain patterns, instability |
| 2. Plain Xray | AP & Lateral views | Check for obvious gaps or hardware issues |
| 3. CT Scan | Thinslice 3D reconstruction | Visualize bone bridge, assess fusion mass |
| 4. FlexionExtension Films | Dynamic Xrays | Detect motion at the fusion site |
| 5. Labs | CRP, ESR, Calcium, Vitamin D | Rule out infection/metabolic causes |
Treatment Options
When Watchful Waiting Works
Not every pseudojoint needs immediate surgery. In mild cases where pain is manageable, doctors may recommend activity modification, a lumbar brace, and physical therapy focused on core stabilization. This conservative route can buy time for the body to attempt a delayed fusion.
Pharmacologic Support
NSAIDs help control pain, but excessive use might impair bone healing, so theyre usually limited to short bursts. Bonestimulating agents like teriparatide (a synthetic PTH) have shown promise in encouraging spinal fusion in osteoporotic patients.
Minimally Invasive Interventions
Techniques such as percutaneous bone graft injection or the use of recombinant bone morphogenetic protein (BMP2) can boost bone growth without a full open revision. These options are especially useful for patients who cant tolerate a long surgery.
Revision Surgery
If pain is severe or the pseudojoint threatens neurological structures, a revision fusion is often the definitive fix. Surgeons may remove loose hardware, place fresh autograft or allograft bone, and add interbody cages to restore disc height and stability. For patients tracking recovery and longterm outcomes after spinal problems, understanding osteoporosis rehab principles can be helpful when planning postoperative rehabilitation and fall-prevention strategies.
Pros & Cons Table
| Treatment | Success Rate | Recovery Time | Complication Risk |
|---|---|---|---|
| Watchful Waiting | 3040% (pain relief) | Weeksmonths | Low |
| BoneStimulating Drugs | 4555% (fusion promotion) | 36 months | Moderate (sideeffects) |
| Minimally Invasive Graft | 6070% (fusion) | 24 months | LowModerate |
| Revision Fusion Surgery | 8090% (solid fusion) | 612 months | Higher (infection, hardware failure) |
Outcomes & Disability
Functional Impact
When a pseudojoint stays untreated, chronic pain can limit daily activities, affect work performance, and reduce quality of life. Many patients report difficulty sitting for long periods, climbing stairs, or lifting even light objects.
Legal & Insurance Considerations
In the U.S., the Social Security Administration classifies severe, persistent spinal pseudarthrosis as a potential disability if it prevents the individual from performing substantial gainful activity. Documentation from an orthopedic surgeon, imaging, and functional assessments are essential for filing a claim.
Prognosis After Successful Fusion
When a solid fusion is finally achieved, most patients experience a dramatic drop in painoften >70% improvement within the first six months. Return-to-work timelines vary: sedentary jobs may resume in 812 weeks, while physically demanding occupations can take 46 months.
PatientStory Box
I was 42, had a lumbar fusion at L5S1, and three months later my back still ached. The surgeon told me Id developed pseudarthrosis. After a revision surgery with BMP2, I was painfree within two months and could finally walk my dog again without wincing. Mark, 2022 patient.
Prevention Tips
PreOperative Optimization
Quit smoking at least six weeks before surgery, keep blood sugar under control, and ensure adequate vitamin D and calcium levels. Even a short prehab program focusing on core strength can make a massive difference.
Surgical Best Practices
Surgeons aim for meticulous decortication (scraping the bone surface), use a robust graft mix (autograft + allograft), and position hardware to distribute load evenly. Some centers now apply intraoperative CT to verify graft placement before closing.
PostOperative Care
Early mobilizationunder the watchful eye of a physical therapisthelps stimulate bone healing. Wearing a lumbar brace for the first 68 weeks provides extra stability while the fusion matures.
Prevention Checklist (Downloadable PDF)
- Stop smoking 6weeks before surgery
- Check vitamin D level Target >30ng/mL
- Maintain blood glucose <130mg/dL
- Engage in prehab core exercises (1015min/day)
- Follow surgeons postop bracing schedule
Key Takeaways
To sum it all up, pseudarthrosis is a false joint that can arise after a fracture or spinal fusion, most commonly at the lumbar L5S1 level. Recognizing its hallmark symptomssharp, persistent pain and a sense of instabilityhelps you seek timely imaging (CT, dynamic Xray) and accurate diagnosis. Treatment ranges from careful observation and medication to minimally invasive grafts and, when needed, revision surgery. Prevention is a team effort: quit smoking, optimize nutrition, and follow your surgeons rehab plan. If you suspect pseudarthrosis, dont waittalk to a spine specialist, get the proper scans, and explore the options that fit your lifestyle and goals.
Got questions about your own back pain or want to share how youve tackled a tough recovery? Drop a comment below or reach out to a trusted healthcare professional. Remember, youre not alone in this journeyknowledge and a supportive community can turn a painful false joint into a stepping stone toward a healthier, stronger you.
FAQs
What causes pseudarthrosis after spinal fusion?
Pseudarthrosis can result from factors like smoking, poor blood sugar control, inadequate bone graft material, infection, or insufficient blood supply to the fusion site.
How is pseudarthrosis diagnosed?
Diagnosis typically involves a combination of clinical examination, plain X‑rays, CT scans for bone continuity, flexion‑extension X‑rays to show motion, and lab tests to rule out infection.
What treatment options are available for pseudarthrosis?
Options range from conservative management (brace, physical therapy) and bone‑stimulating medications to minimally invasive bone graft injections and, when needed, revision fusion surgery.
Can pseudarthrosis be prevented?
Yes—quitting smoking, optimizing vitamin D and calcium levels, controlling diabetes, using proper surgical techniques, and adhering to post‑op rehabilitation protocols all lower the risk.
When should I seek urgent medical attention for pseudarthrosis?
Urgent care is needed if you experience sudden neurological deficits (numbness, weakness), loss of bladder or bowel control, or a rapid increase in pain after a minor fall.