If youve been told you have ankylosing spondylitis (AS) and suddenly feel a nagging ache in your shoulder, youre probably wondering, Is this part of the disease or just a random injury? The short answer: yes, shoulder pain can be a direct offshoot of AS, and catching it early can save you from a lot of frustration later on. Below, well break down why it happens, how doctors spot it, what you can actually do at home, and when its time to call in the specialists. Think of this as a chat over coffeeno jargon, just honest advice and a few practical tips you can try right now.
Understanding the Connection
How common is shoulder pain in ankylosing spondylitis?
Studies suggest that roughly onethird of people living with AS report some form of shoulder discomfort at some point to Healthline. That number may sound high, but it makes sense when you consider how AS loves to target the places where bones, tendons, and ligaments meetcalled entheses. The shoulder, with its many moving parts, is a prime spot for inflammation to set up shop. If youre trying to understand longterm goals like ankylosing spondylitis remission, tracking peripheral joint symptoms such as shoulder pain can be a helpful marker.
Statistics Overview
| Study | Population | Shoulder Pain Prevalence |
|---|---|---|
| Healthline Review (2023) | 1,200 AS patients | 33% |
| Reumatologia Clinica (2022) | 487 AS patients | 29% |
| American College of Rheumatology Survey (2024) | 2,030 AS patients | 35% |
Which shoulder structures get hit first?
In AS, the most frequent culprits are the acromioclavicular (AC) joint and the rotatorcuff tendons. The inflammation can also spread to the glenohumeral capsule, making the whole joint feel stiff, achy, and less willing to cooperate when you try to lift a grocery bag.
How does ASrelated shoulder pain differ from a regular sore shoulder?
Typical mechanical shoulder painthink of a rotatorcuff tearusually follows a specific injury, gets worse with certain movements, and often spikes at night. ASrelated pain, on the other hand, tends to be more diffuse, may be present on both sides, and often worsens after periods of inactivity (like after a long bingewatching session). If you notice that your shoulder aches right after a stiff day at the office, thats a clue its linked to your spine disease rather than a strained muscle.
Redflag signs that need urgent attention
- Sudden, severe night pain that wakes you up.
- Rapid loss of motion (you cant raise your arm above shoulder height).
- Visible swelling, warmth, or fever.
- Sharp, stabbing pain after a minor bumpcould indicate a fracture.
When any of these appear, its best to schedule an appointment with your rheumatologist or orthopedist ASAP.
Diagnosing Shoulder Involvement
Which imaging tests reveal shoulder problems?
Three main tools are on the table: plain Xrays, magnetic resonance imaging (MRI), and ultrasound. Xrays are great for spotting boneonbone changes in the AC joint, while MRI can show early inflammation in the soft tissues before any bony damage occurs. Ultrasound is handy for realtime assessment and can even guide a steroid injection if needed.
Modality Comparison
| Modality | What It Shows | When Its Used |
|---|---|---|
| Xray | Joint space narrowing, bone spurs | Firstline, low cost |
| MRI | Softtissue inflammation, early erosions | Persistent pain, unclear Xray |
| Ultrasound | Synovial fluid, tendon integrity | Guided injections, bedside |
When is a plain Xray enough?
If youre in the early stages of disease and the pain feels mild, an Xray of the shoulder can often reveal the telltale narrowing of the AC joint space. Thats usually sufficient to confirm that the shoulder is part of the AS picture, especially when combined with a clinical exam.
Role of MRI and ultrasound
MRI shines when the Xray looks normal but you still have pain. It can pick up fluid accumulation and bone marrow edemaearly signs that the disease is lighting up the shoulder before the bones speak. Ultrasound, meanwhile, is a quick, radiationfree way to see if theres bursitis or tendonitis, and it can help your doctor place a corticosteroid shot with pinpoint accuracy.
Do blood tests help?
Elevated ESR (erythrocyte sedimentation rate) or CRP (Creactive protein) often accompany active inflammation, but theyre not specific to the shoulder. A positive HLAB27 test can reinforce the AS diagnosis, especially if youre still on the fence about whether shoulder pain is part of the disease.
Other conditions that mimic AS shoulder pain
Its easy to confuse ASrelated pain with rotatorcuff tears, frozen shoulder (adhesive capsulitis), or simple osteoarthritis. A quick comparative chart can help you selfscreen, but remember: a definitive diagnosis always needs a professional eye.
Quick Comparison
| Condition | Typical Pain Pattern | Key Distinguishing Feature |
|---|---|---|
| AS Shoulder Involvement | Diffuse, bilateral, worse after inactivity | Associated spine stiffness |
| RotatorCuff Tear | Sharp, especially with overhead motion | History of trauma |
| Frozen Shoulder | Progressive loss of motion in all directions | Night pain, capsular thickening on MRI |
| Osteoarthritis | Deep ache, crepitus | Joint space narrowing on Xray |
Managing Shoulder Pain
Can I treat shoulder pain at home without medication?
Absolutely. Gentle movement, heat or ice therapy, and posture tweaks can do wonders for earlystage discomfort. The key is to stay activenot to force the shoulder, but to keep the joint lubricated and the surrounding muscles strong enough to protect it.
Top 5 shoulderankylosisprevention exercises
These moves are lowimpact, easy to fit into a morning routine, and they address the muscles that keep your shoulder from locking up.
- Pendulum Swing: Lean forward, let your arm dangle, and gently swing it in small circles for 30 seconds each direction.
- Scapular Retractions: Sit or stand tall, pinch shoulder blades together, hold 5 seconds, repeat 10 times.
- Doorframe Stretch: Place forearms on a doorway, step forward until you feel a light stretch across the front of the shoulders, hold 20 seconds.
- Wall Angels: Back against a wall, arms at 90, slide them up and down like a snow angel2 sets of 10.
- Band External Rotations: Attach a resistance band to a stable point, keep elbow at 90, rotate the forearm outward2 sets of 12.
Doing these daily can help you stay mobile, especially if youre in ankylosing spondylitis stage4 where stiffness is a bigger threat.
When are corticosteroid injections appropriate?
If NSAIDs and exercises havent tamed the flare, a guided steroid shot into the AC joint or subacromial space can bring rapid relief. Its not a cureall, but it can buy you weeks of calmer days while you work on strengthening the surrounding muscles.
Pros vs. Cons
| Pros | Cons |
|---|---|
| Fast pain relief (often within 2448hrs) | Possible temporary increase in blood sugar for diabetics |
| Reduces inflammation locally | Repeated injections may weaken tendons over time |
| Can delay need for oral steroids | Risk of infection if not done aseptically |
Which medications work best for shoulder pain in AS?
Firstline treatment remains NSAIDs (like ibuprofen or naproxen). If pain persists, biologic agents that target TNF or IL17 pathwayssuch as adalimumab or secukinumabhave shown to reduce peripheral joint inflammation, including the shoulder. Always discuss dosage and sideeffects with your rheumatologist before starting. For guidance on how clinicians define treatment goals, see discussion of AS remission criteria which can shape decisions about stepping up to biologics.
How to stay active without overloading the shoulder?
Lowimpact cardiovascular activitiesswimming, brisk walking, or stationary cyclingkeep blood flow moving without pounding the joint. Pair those with the shoulderspecific exercises above, and youll maintain both overall fitness and targeted mobility.
Sample Weekly Plan
| Day | Activity |
|---|---|
| Monday | 30min brisk walk + shoulder routine (pendulum, wall angels) |
| Tuesday | Swimming (20min) + band external rotations |
| Wednesday | Rest + gentle stretching |
| Thursday | Stationary bike (30min) + scapular retractions |
| Friday | Yoga for spine (focus on gentle twists) + doorframe stretch |
| Saturday | Light hike (avoid heavy backpack) + full shoulder routine |
| Sunday | Rest or casual stroll |
Stages of AS and the Shoulder
What happens to the shoulder in early vs. advanced stages?
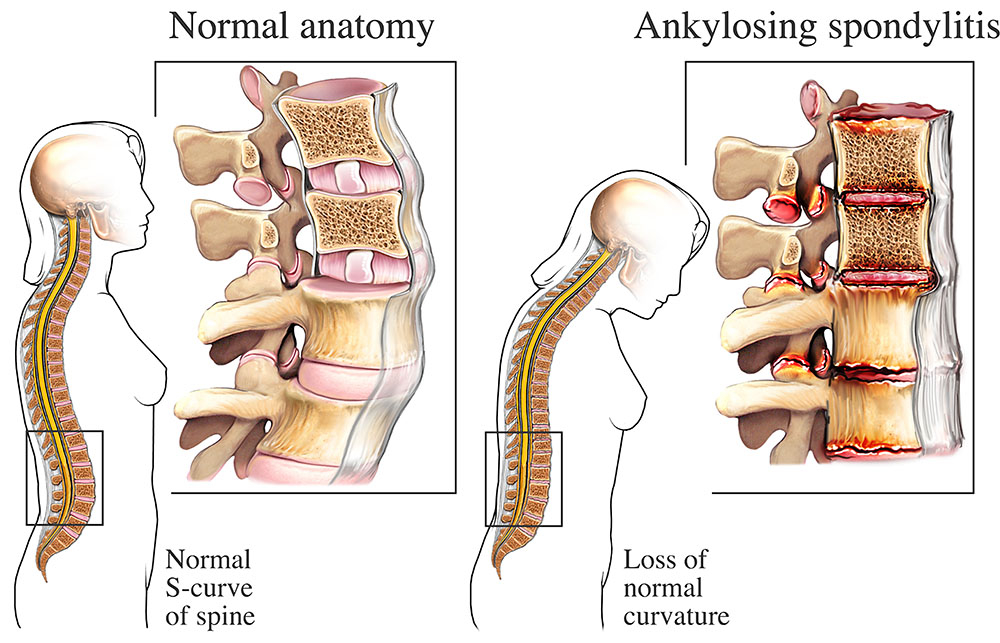
During stage12, imaging may only show subtle softtissue swelling, and shoulder pain is often intermittent. By stage34, bone formation (ankylosis) can start, leading to reduced range of motion and, in severe cases, complete shoulder fusion. The difference is not just academicit influences how aggressively you should pursue physiotherapy and medication.
Can shoulder ankylosis be prevented?
Yes, with a proactive approach. Regular stretching, consistent use of the exercises above, and prompt treatment of flares (NSAIDs or steroids) dramatically lower the odds of permanent stiffening. Think of your shoulder like a hinge: if you oil it regularly, it wont seize up.
Longterm outlook for people with shoulder involvement
Modern biologic therapies have shifted the prognosis dramatically. A 2024 metaanalysis reported that over 80% of patients on TNF inhibitors maintained functional shoulder range of motion after five years to the study. In plain speak: with the right treatment plan, you can keep using your arm to hug, cook, and play with kids well into later life.
Common Questions (Featured Snippet Ready)
Can ankylosing spondylitis cause shoulder pain?
Yesabout onethird of AS patients experience shoulder discomfort, usually due to inflammation of the AC joint or rotatorcuff tendons.
Is shoulder pain a sign of stage4 AS?
Not necessarily. Shoulder pain can appear at any stage, but persistent, worsening pain with loss of motion is more common in later stages.
How can I tell if my shoulder pain is from AS or a rotatorcuff tear?
ASrelated pain is typically bilateral, worse after inactivity, and accompanied by spine stiffness. A rotatorcuff tear often follows a specific injury and spikes with overhead movements.
What is the best exercise to keep my shoulder from stiffening?
Daily wallangel and scapularretraction circuits (2sets10reps) maintain mobility without overloading inflamed tissue.
When should I see a rheumatologist versus an orthopedist?
If the pain comes with systemic flareups or spinal symptoms, start with a rheumatologist. For isolated mechanical issues, an orthopedist can help with imaging and possible injections.
Conclusion
Shoulder pain doesnt have to be a dreaded sideeffect of ankylosing spondylitis. By recognizing the signs early, getting the right imaging, staying active with targeted exercises, and partnering with knowledgeable healthcare providers, you can keep your shoulders flexible and painfree. If youve been dealing with that nagging ache, try one of the simple stretches today and schedule a checkup to discuss whether a biologic or a brief steroid injection might be right for you. Wed love to hear how these tips work for youshare your story in the comments or ask any lingering questions. Your journey can inspire someone else whos just starting to wonder, Whats next for my shoulders?
FAQs
Why does ankylosing spondylitis cause shoulder pain?
AS targets entheses – the attachment sites of tendons, ligaments, and joint capsules. In the shoulder, inflammation often affects the acromioclavicular joint and rotator‑cuff tendons, leading to diffuse ache and stiffness.
How can I tell if my shoulder pain is from AS or a rotator‑cuff tear?
AS‑related pain is usually bilateral, worsens after periods of inactivity, and comes with spinal stiffness. A rotator‑cuff tear typically follows a specific injury and spikes with overhead movements.
What imaging test should I get first for shoulder pain in AS?
Start with a plain X‑ray of the shoulder to look for AC‑joint narrowing or bone spurs. If the X‑ray is normal but pain persists, an MRI or ultrasound can reveal early soft‑tissue inflammation.
Which home exercises are most effective for preventing shoulder stiffness?
Daily pendulum swings, scapular retractions, door‑frame stretches, wall angels, and band external rotations keep the joint lubricated and the surrounding muscles strong.
When is a corticosteroid injection appropriate for AS shoulder pain?
If NSAIDs and exercises haven’t controlled a flare, a guided steroid injection into the AC joint or sub‑acromial space can provide rapid relief and buy time for physiotherapy.