Hey there, I get itliving with ankylosing spondylitis (AS) can feel like youre stuck on a neverending roller coaster of stiffness, pain, and uncertainty. If youre scrolling through endless medical jargon hoping for a clear answer, let me give it to you straight: the best AS therapy is a personalized mix of medicines, movement, and everyday habits that together help you reclaim comfort and mobility.
Below youll find the latest, evidencebacked options (including the newest IL17 and JAK inhibitors), the pros and cons of each, and realworld tips so you can decide whats right for you right now. Ready? Lets dive in.
What Is Ankylosing Spondylitis
Definition and Who Gets It
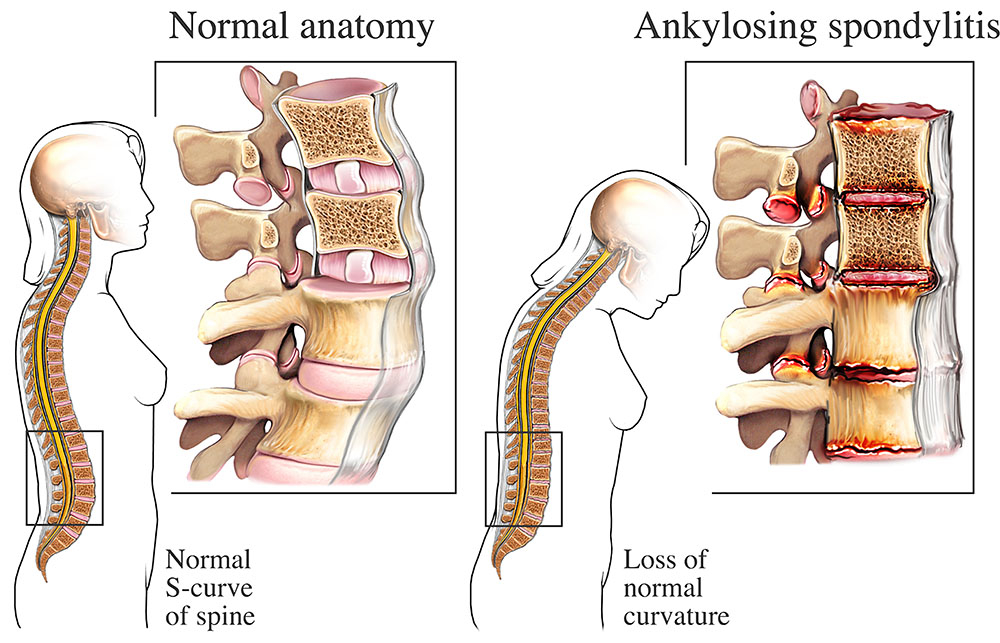
Ankylosing spondylitis is a chronic inflammatory disease that primarily attacks the spine and sacroiliac joints, gradually fusing vertebrae together. It usually shows up in early adulthood, but anyone can be affected. According to the , about 1.3% of the population worldwide lives with this condition.
Symptoms in Women
While men often experience classic lowerback pain, women may notice more peripheral joint pain, fatigue, and even heel inflammation. These ankylosing spondylitis symptoms females can sometimes delay diagnosis because they dont fit the textbook picture.
Understanding Stage4
When AS reaches stage4, the spine has significant fusion, limiting flexibility and sometimes causing a forwardleaning posture. At this point, therapy shifts from solely slowing progression to preserving function, relieving pain, and preventing complications like fractures.
How Its Diagnosed
Diagnosis typically combines a physical exam, imaging (Xray or MRI), and blood tests for HLAB27. A rheumatologist will use scoring tools like BASDAI to gauge disease activity. Early and accurate ankylosing spondylitis criteria is crucial because it opens the door to effective therapy before irreversible damage occurs.
Core Therapy Pillars
Medication Options
| Therapy | How It Works | Typical Dose & Route | Main Benefits | Common SideEffects / Risks |
|---|---|---|---|---|
| NSAIDs (ibuprofen, naproxen) | COX inhibition inflammation | Oral, 23/day | Fast pain relief, firstline | GI irritation, renal caution |
| AntiTNF biologics (adalimumab, etanercept) | Blocks TNF cytokine | SubQ injection, every 12weeks | Strong diseaseactivity reduction | Infection risk, injection reactions |
| IL17 inhibitors (secukinumab, ixekizumab) | Targets IL17A cytokine | SubQ loading then monthly | Effective for TNFfailures | Candida infections, mild neutropenia |
| JAK inhibitors (upadacitinib, filgotinib) | Inhibits JAK pathways cytokine signaling | Oral, daily | Convenient oral option, rapid response | Thrombosis risk, lab monitoring needed |
| DMARDs (sulfasalazine) | Immunomodulation (peripheral joints) | Oral, twice daily | Helpful if peripheral arthritis present | Nausea, liver monitoring |
When you hear phrases like best medicine for ankylosing spondylitis or what is the latest treatment for ankylosing spondylitis, the reality is that each option fits different disease stages and personal health profiles. A rheumatologist can guide you toward the most suitable ankylosing spondylitis therapy based on severity, comorbidities, and lifestyle.
NonDrug Therapies
Medication alone isnt the whole story. Think of nondrug strategies as the supporting cast that keep your spine moving and your spirit up.
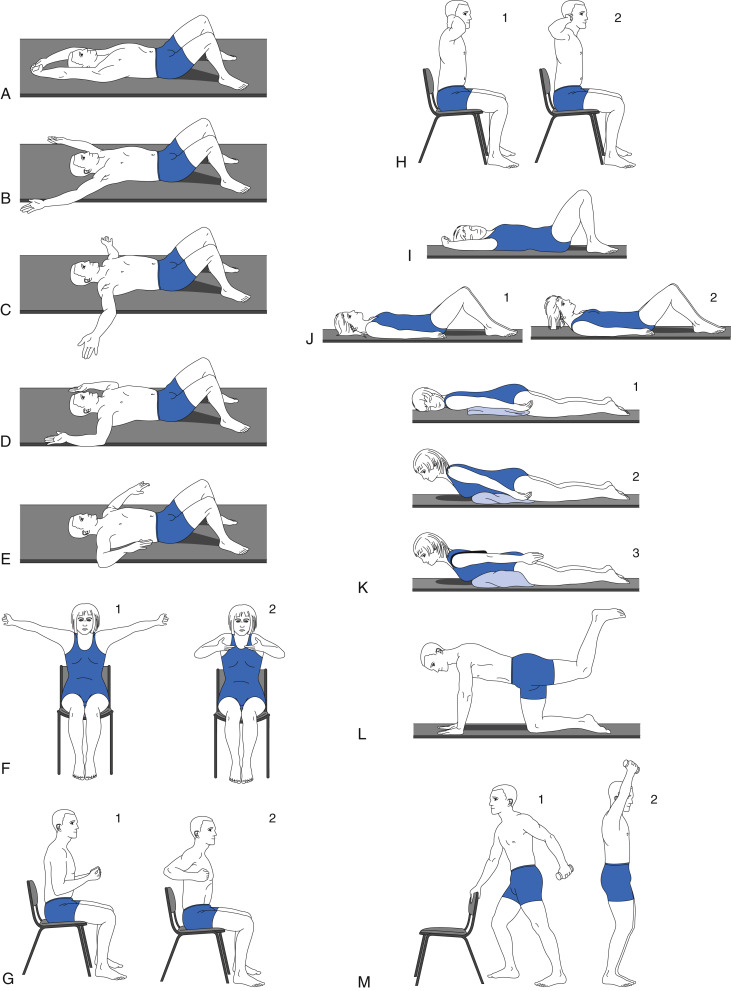
- Physical therapy & exercise Corestrengthening, gentle stretching, and lowimpact cardio (swimming, cycling) improve flexibility. A certified physiotherapist often prescribes a 3timesweekly routine that gradually intensifies.
- Posture & ergonomics Simple habits like sitting with a lumbar roll, standing tall, and avoiding prolonged slouching can reduce mechanical stress on the spine.
- Heat & cold therapy Warm showers or heating pads ease muscle tightness, while ice packs can calm acute inflammation after a flare.
- Surgery Reserved for advanced stage4 cases where vertebral fusion or hip arthritis causes severe pain or functional loss. Procedures range from spinal osteotomy to hip replacement.
Lifestyle & SelfManagement
Even the best treatment for spondylitis can be undermined by daily choices. Here are a few loweffort tweaks that make a big difference:
- Nutrition Antiinflammatory foods (fatty fish, leafy greens, turmeric) plus adequate VitaminD and calcium support bone health.
- Quit smoking Smoking accelerates spinal damage and reduces medication effectiveness.
- Stress reduction Mindbody practices like meditation or gentle yoga lower systemic inflammation.
Choosing Your Treatment
Assessing Disease Activity
Before any plan, your rheumatologist will gauge activity using the BASDAI score, MRI findings, and blood markers (CRP, ESR). Higher scores often call for stronger biologics, while milder activity might be managed with NSAIDs and exercise alone.
Personal Factors Matter
Age, gender, other health conditions, and even family planning can tip the scales. For example, women who are pregnant may avoid certain biologics and instead rely more heavily on physical therapy and carefully selected NSAIDs.
Cost & Access
Biologics can be pricey, but many manufacturers offer patientassistance programs. Its worth chatting with your insurance coordinator and exploring coupons or nonprofit support.
Safety Monitoring
Every medication requires a safety net. Typical labs include CBC, liver enzymes, and TB screening before starting biologics. Followup visits every 36 months keep you and your doctor on the same page.
DecisionMaking Toolkit
Grab a printable questionnaire (downloadable PDF) that helps you rank what matters mostpain relief, sideeffect profile, convenience, or cost. As the American College of Rheumatologys 2024 guideline stresses, shared decisionmaking is key to longterm adherence.
Real Success Stories
Sarahs Journey FemaleSpecific Symptoms
Sarah, a 32yearold graphic designer, first noticed unexplained heel pain and chronic fatigue. After an MRI revealed sacroiliitis, she was diagnosed with AS. Her rheumatologist started her on an IL17 inhibitor combined with a tailored physiotherapy program. Within six months, Sarahs morning stiffness dropped from two hours to under fifteen minutes. I still have flareups, she says, but I can finally walk my dog without fearing a collapse.
Johns Battle Stage4 Management
John, 58, waited too long to seek help. By the time he was diagnosed, his spine had fused in a forwardleaning posture (stage4). He underwent spinal osteotomy surgery followed by a regimen of antiTNF biologics and daily swimming. Today, John can attend his grandsons soccer gamesa feat he thought impossible a year ago.
Debunking How I Cured My Ankylosing Spondylitis
There are countless stories online promising a permanent cure for ankylosing spondylitis. While its tempting to believe in a miracle, the medical consensus says theres no permanent cureonly effective therapy that can halt progression and dramatically improve quality of life. Sharing realistic expectations builds trust and prevents disappointment. For those interested in defining remission, reviewing the AS remission criteria can provide useful insight into treatment goals and disease control.
Bottom Line Checklist Your Personal Ankylosing Spondylitis Therapy Plan
- Confirm diagnosis and disease stage (refer to NIAMS or your rheumatologist).
- Discuss medication optionsNSAIDs, biologics, or JAK inhibitorsbased on activity level.
- Start a supervised exercise program within two weeks (core strengthening, stretching, lowimpact cardio).
- Set up a lab and monitoring schedule (baseline labs, then every 3 months).
- Review lifestyle factorsquit smoking, adopt antiinflammatory diet, manage stress.
- Reevaluate every six months; adjust therapy as needed.
Feel free to download the printable version of this checklist and keep it on your fridge as a daily reminder.
Conclusion
Living with ankylosing spondylitis doesnt have to be a life sentence of pain and limitation. By combining the right ankylosing spondylitis therapywhether thats the latest IL17 inhibitor, a consistent physiotherapy routine, or simple lifestyle tweaksyou can slow disease progression, reclaim mobility, and enjoy the moments that matter.
Weve covered the science, the options, and real stories from people just like you. Now its your turn: What part of the therapy plan resonates most with you? Have you tried a specific exercise or medication that made a difference? Share your experiences in the comments, and lets keep supporting each other on this journey. If you have any questions, dont hesitate to askyour next step toward relief might be just a conversation away.
FAQs
What are the first‑line medications for ankylosing spondylitis?
Non‑steroidal anti‑inflammatory drugs (NSAIDs) such as ibuprofen or naproxen are usually tried first because they reduce pain and inflammation quickly and are inexpensive.
How do IL‑17 inhibitors differ from anti‑TNF biologics?
IL‑17 inhibitors (e.g., secukinumab, ixekizumab) target the interleukin‑17 pathway, which can be effective for patients who don’t respond to anti‑TNF agents that block tumor‑necrosis factor‑α. Their side‑effect profile also differs, with a higher risk of mild fungal infections.
Can exercise really slow the progression of ankylosing spondylitis?
Yes. Regular, supervised physiotherapy and low‑impact activities (swimming, cycling, stretching) maintain spinal flexibility, improve posture, and may delay vertebral fusion when combined with appropriate medication.
What lifestyle changes have the biggest impact on AS symptoms?
Quitting smoking, eating an anti‑inflammatory diet rich in omega‑3 fatty acids, maintaining adequate vitamin D and calcium, and managing stress through meditation or gentle yoga all help reduce systemic inflammation and support bone health.
Are JAK inhibitors safe for long‑term use in ankylosing spondylitis?
JAK inhibitors (e.g., upadacitinib) are oral and effective, but they require regular lab monitoring because they can increase the risk of blood clots, infections, and changes in cholesterol. Discuss the risk‑benefit balance with your rheumatologist.