Looking for the lowdown on the eular pmr guidelines? Youve come to the right spot. In the next few minutes Ill break down what the latest recommendations say, how they affect your treatment plan, and why striking the right balance between benefits and risks matters. Think of this as a friendly coffeechat with a knowledgeable buddy whos been through the same maze.
Why Guidelines Matter
The European League Against Rheumatism (EULAR) teamed up with the American College of Rheumatology (ACR) to craft a set of evidencebased rules for managing polymyalgia rheumatica (PMR). Why should you care? Because a clear, shared roadmap means doctors can start the right therapy sooner, avoid unnecessary sideeffects, and keep you feeling yourself.
These guidelines arent just a list of bullet points; theyre the result of dozens of rheumatologists, epidemiologists, and patientadvocates poring over years of data. The 2025 update builds on the original 2015 version, tightening the glucocorticoid taper schedule, adding recommendations for bone health monitoring, and highlighting redflag symptoms that could signal giantcell arteritis (GCA). If youve ever felt tossed between conflicting advice, the guidelines are the place to find consensus.
Core Recommendations
How should glucocorticoids be started?
Think of glucocorticoids as the starter pistol for PMRfast, effective, but needing careful handling. The guideline suggests beginning with 1520mg of prednisoneequivalent daily for most patients. This dose often relieves shoulder and hip girdle pain within a few days. If youre a lightweight or have diabetes, your doctor might start a bit lower and adjust quickly.
Whats the tapering plan?
Longterm steroid use is a doubleedged sword. The eular pmr guidelines propose a stepdown over 1224months, aiming for the lowest dose that still controls symptoms. A typical approach looks like this:
| Month | Prednisone Dose (mg) |
|---|---|
| 02 | 1520 |
| 34 | 1012 |
| 56 | 79 |
| 79 | 56 |
| 1012 | 24 |
| 1324 | 2 (or stop) |
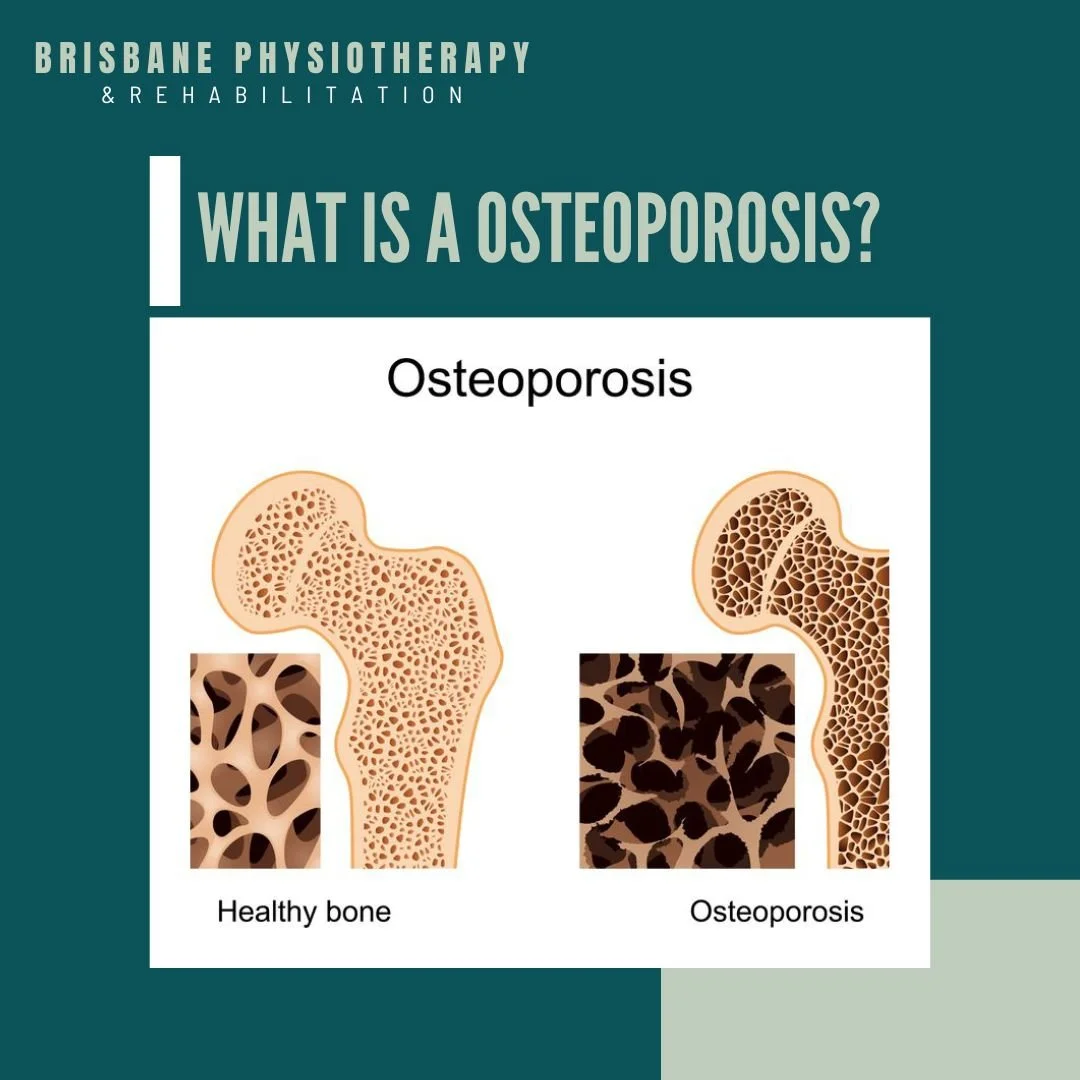
Never rush the taper; sudden drops raise the risk of flareups. Your doctor will check your ESR or CRP levels and ask about morning stiffness to decide if its safe to cut the dose further. If steroid therapy raises concerns about bone health, consider pairing this plan with targeted osteoporosis physical therapy measures to help preserve mobility and reduce fracture risk.
When are DMARDs or biologics on the table?
Glucocorticoids are firstline, but if you experience repeated flares, steroidinduced osteoporosis, or uncontrolled blood sugar, the guidelines suggest adding a diseasemodifying antirheumatic drug (DMARD) such as methotrexate. Biologics are still a last resort for PMR, reserved for patients with concurrent giantcell arteritis or those who simply cant taper steroids without severe relapse.
What monitoring is required?
Regular checkins keep the treatment on track. The eular pmr guidelines recommend:
- Blood tests every 23months (CRP, ESR, fasting glucose, lipid profile).
- Bone density scan (DEXA) at baseline, then every 12months if you stay on steroids.
- Blood pressure and weight checkssteroids can raise both.
- Patientreported outcomes like the visualanalogue pain scale at each visit.
How to spot GCA overlap?
Giantcell arteritis can hide behind PMR symptoms, but its a medical emergency. Redflag signs include newonset headache, scalp tenderness, visual disturbances, or jaw claudication. If any of these appear, the guideline advises immediate highdose steroids and an urgent referralthink of it as pulling the fire alarm in a building.
Practical Tools
Because guidance is great, but implementation can feel like assembling IKEA furniture without instructions, here are some handy resources you can actually use.
Downloadable taper calculator
Weve built a simple Google Sheet (free to copy) that lets you plug in your starting dose and automatically generates a monthbymonth taper schedule. Its an easy way to visualize the journey and share the plan with your clinician.
Checklist for GCA warning signs
Print this concise list and keep it on your fridge:
- Sudden headache or scalp pain?
- Blurred vision or double vision?
- Jaw pain while chewing?
- Fever >38C without infection?
If you tick any box, call your doctor right away.
Patientfriendly PDF summary
Just like the guidelines offer a clean, printable version for RA, you can request a onepage PMR cheat sheet from your rheumatology clinic. It distills the key points into bullet form, perfect for quick reference before appointments.
Comparing other EULAR guidelines
While youre here, you might wonder how PMR fits into the larger rheumatology landscape. Below is a quick snapshot of related guidelines:
| Condition | Key Guideline Document | Year |
|---|---|---|
| Rheumatoid arthritis | 2022 | |
| Psoriatic arthritis | 2021 | |
| Osteoarthritis (knee) | 2020 | |
| Systemic lupus erythematosus | 2023 | |
| Vasculitis | 2021 |
Seeing the bigger picture helps you appreciate why consistency across diseases mattersespecially when you, as a patient, might have more than one rheumatic condition.
Benefits & Risks
Clinical benefits of following the guideline
Sticking to the eular pmr guidelines typically leads to faster pain relief, fewer flares, and a more predictable disease course. In a 2023 Norwegian cohort study, 82% of patients who adhered to the taper algorithm achieved remission within 12months, compared with just 55% who deviated.
Potential adverse effects
Glucocorticoids can be a bit of a villain when used longterm. Common sideeffects include:
- Osteoporosis and fractures.
- Elevated blood sugar diabetes risk.
- Increased susceptibility to infections.
- Mood swings or insomnia.
How to mitigate risks
Prevention is easier than cure. The guideline suggests:
- Calcium (1,0001,200mg) plus vitaminD (8001,000IU) daily.
- Bonepreserving agents such as bisphosphonates for anyone on steroids >3months.
- Regular exercisestrength training helps keep your joints supple and your bones strong.
- Early glucose monitoring if you have a family history of diabetes.
When to deviate from the guideline
No rule is absolute. Your physician may adjust the plan if you have:
- Severe liver or kidney disease.
- Active peptic ulcer disease.
- Personal preference after a shareddecision discussion.
In those cases, transparent communication is keylet your doctor know your concerns, and ask for a rationale behind any change.
Staying Updated
Medical knowledge evolves, and the EULAR task force is already sketching the next edition of the PMR guidance. Heres how you can stay in the loop:
- Subscribe to the for quarterly updates.
- Follow the official EULAR Twitter handle @EULAR_Rheumatology.
- Join patientfocused webinarsmany are free and feature rheumatologists discussing realworld case studies.
- If youre interested in research, consider enrolling in a clinical trial exploring steroidsparing agents (search ClinicalTrials.gov for PMR trials).
Being proactive not only empowers you, it also gives your healthcare team a clearer picture of your expectations.
Conclusion
The eular pmr guidelines give us a clear, evidencebacked roadmap: start with a reasonable steroid dose, taper thoughtfully over 1224months, monitor closely for sideeffects, and stay alert for giantcell arteritis. By weighing the clear benefits against the possible risksand using the practical tools weve highlightedyou can navigate PMR treatment with confidence and peace of mind.
Have you tried the taper calculator or found a helpful checklist? Share your experience in the comments below, and lets keep this conversation going. If you have any lingering questions, feel free to askyour journey matters, and were all in this together.
FAQs
What is the recommended starting dose of prednisone for PMR according to the 2025 guidelines?
The guidelines suggest beginning with 15–20 mg of prednisone‑equivalent daily for most patients, adjusting lower for those who are lightweight or have diabetes.
How long should the glucocorticoid taper last, and what is a typical schedule?
The taper is planned over 12–24 months, aiming for the lowest dose that controls symptoms. A common schedule reduces the dose stepwise every 2–3 months, ending at ≤2 mg or stopping by month 24.
When should a DMARD or biologic be considered in PMR management?
DMARDs like methotrexate are added if patients have repeated flares, steroid‑induced osteoporosis, or uncontrolled blood sugar. Biologics are reserved for refractory cases or when giant‑cell arteritis co‑exists.
What monitoring tests are recommended during steroid therapy?
Blood tests (CRP, ESR, fasting glucose, lipids) every 2–3 months, a baseline DEXA scan with annual repeats if steroids continue, plus regular blood pressure, weight, and patient‑reported pain assessments.
What are the red‑flag symptoms that suggest overlapping giant‑cell arteritis?
New‑onset headache, scalp tenderness, visual disturbances, jaw claudication, or fever > 38 °C without infection require immediate high‑dose steroids and urgent referral.