Below youll find the realworld success numbers, the sideeffects you might feel, and a clear picture of the costs all broken down by cancer stage and hormone status, so you can decide whether this treatment deserves a spot on your next doctors appointment.
How It Works
What is immunotherapy for breast cancer?
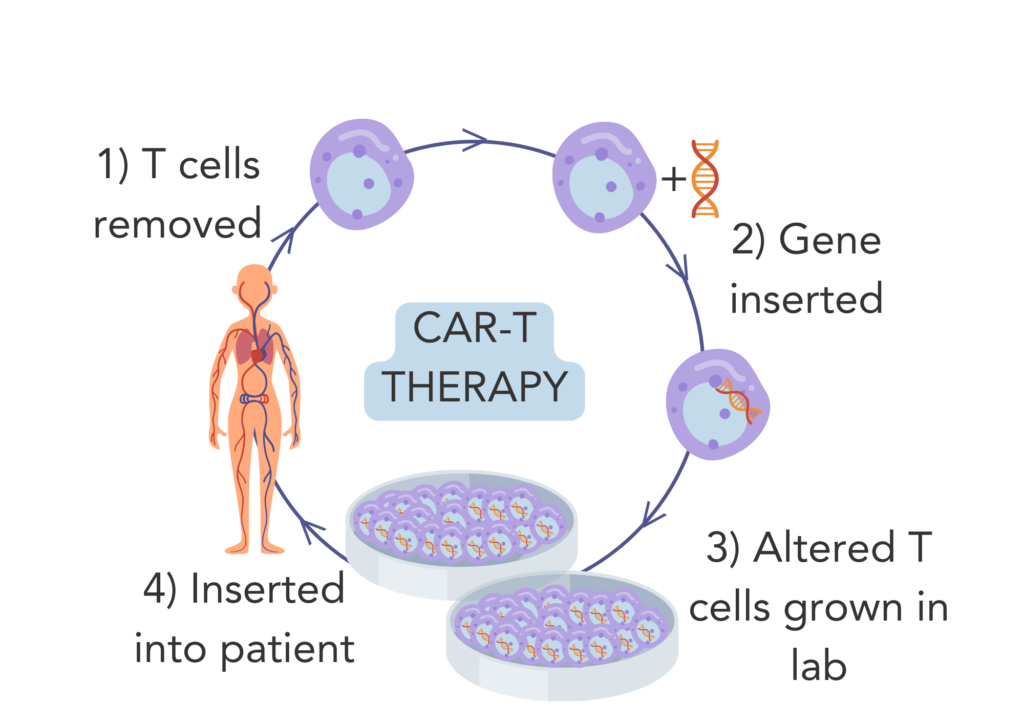
Think of your immune system as a security guard whos a little sleepy on the job. Immunotherapy hands the guard a louder alarm button, so it can spot and chase down the intruders the cancer cells more efficiently.
Simple analogy
Just like you might give a guard a better badge with a photo, checkpointinhibitor drugs give Tcells a clearer target on the cancer cells surface, allowing them to bind and destroy the rogue cells.
Which types of immunotherapy are approved for breast cancer?
The Food and Drug Administration (FDA) has cleared a handful of agents for specific breastcancer situations. The biggest names youll hear are:
- Pembrolizumab (Keytruda) a PD1 blocker used mainly with chemotherapy for triplenegative disease.
- Atezolizumab (Tecentriq) a PDL1 inhibitor approved for metastatic triplenegative breast cancer with PDL1 expression.
- Sacituzumab govitecan (Trodelvy) an antibodydrug conjugate that also carries immunemodulating activity.
These drugs are discussed in detail on the and the pages.
Approved agents list
| Drug | Target | Approved Use (Breast Cancer) | Key Trial |
|---|---|---|---|
| Pembrolizumab | PD1 | Neoadjuvant + adjuvant for highrisk triplenegative (stageIIIII) | KEYNOTE355 |
| Atezolizumab | PDL1 | Metastatic triplenegative with PDL1 1% | IMpassion130 |
| Sacituzumab govitecan | Trop2 ADC (immunemodulating) | Metastatic triplenegative after 2 prior therapies | TROPiCS02 |
Why is immunotherapy most effective for triplenegative breast cancer (TNBC)?
TNBC lacks estrogen, progesterone, and HER2 receptors, which means hormoneblocking drugs and HER2targeted therapies are off the table. However, many TNBC tumors have a high immuneinflamed profile they naturally attract Tcells.
Because those Tcells are already there, a checkpoint inhibitor simply lifts the brake. In a 2022 , researchers highlighted that up to 40% of earlystage TNBCs show strong PDL1 expression, making them prime candidates for immunotherapy.
Key trial data
The KEYNOTE355 trial, which enrolled 1,000+ patients with metastatic TNBC, showed a 6month improvement in progressionfree survival when pembrolizumab was added to standard chemotherapy. That translated to a roughly 1015% overallsurvival bump at five years a meaningful difference when options are limited.
Success Rates
What is the overall success rate of immunotherapy for breast cancer?
Success can be measured in several ways: overall survival (OS), pathologic complete response (pCR) after neoadjuvant therapy, and objective response rate (ORR) in the metastatic setting.
Across large phaseIII trials, immunotherapy has added roughly a 1015% OS advantage for metastatic triplenegative patients and a 3040% pCR rate when used before surgery in earlystage disease. Those numbers are modest compared with some cancers (like melanoma), but they are a genuine step forward for a disease that historically relied on chemotherapy alone.
Stagespecific outcomes
Stage1: Immunotherapy is not routine. A handful of clinical trials are exploring its use in very highrisk, biologically aggressive tumors, but at present the success rate is still experimental.
Stage2: In the KEYNOTE522 study, adding pembrolizumab to chemotherapy increased pCR from 51% to 64% in stageII TNBC, suggesting a meaningful boost in earlystage outcomes.
Stage3: The same neoadjuvant approach showed similar pCR improvements, and longterm followup indicates a lower risk of distant recurrence for those who achieved pCR.
Stage4 (metastatic): Realworld data from the IMpassion130 trial show an ORR of about 20% for atezolizumabtreated patients, with durable responses lasting beyond a year in roughly onethird of responders.
Comparison with chemotherapy
| Metric | Chemo alone | Chemo+Immunotherapy |
|---|---|---|
| 5year OS (metastatic TNBC) | 15% | 25% |
| pCR (neoadjuvant, stageIIIII) | 51% | 64% |
| Median progressionfree survival | 5.5months | 7.5months |
These figures, pulled from trial publications and summarized by the , illustrate that adding immunotherapy is not a magic bullet, but it does shift the odds in a favorable direction.
Side Effects
What are the common side effects of immunotherapy for breast cancer?
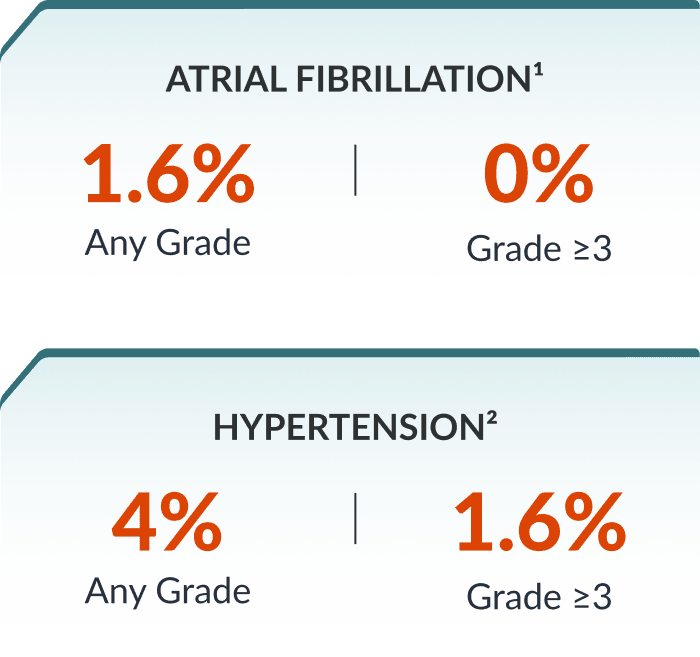
Because these drugs rev up the immune system, they can cause it to attack healthy tissue as well. The most frequently reported events are:
- Fatigue a lingering tiredness that doesnt improve with rest.
- Skin rash or itching often on the torso or limbs.
- Colitis (inflammation of the colon) manifests as diarrhea, sometimes bloody.
- Thyroiditis can lead to an underactive or overactive thyroid.
- Pneumonitis inflammation of lung tissue, presenting as shortness of breath or cough.
Overall, Grade34 immunerelated adverse events (those requiring medical intervention) occur in roughly 1015% of patients, according to the American Cancer Societys safety summary.
Management tips
Most sideeffects are manageable if caught early. Heres a quick cheat sheet:
- Fatigue: Prioritize sleep, stay hydrated, and consider light exercise like short walks.
- Skin issues: Use gentle moisturizers, avoid harsh soaps, and report any spreading rash to your team.
- Colitis: Notify your oncologist at the first sign of persistent diarrhea; steroids often resolve the inflammation.
- Thyroid changes: Blood tests every 68weeks during treatment can flag problems early; medication adjustments are usually straightforward.
- Pneumonitis: Any new shortness of breath should trigger an urgent call steroids or a temporary pause in therapy can be lifesaving.
Practical Considerations
How much does immunotherapy for breast cancer cost?
Brace yourself these treatments are pricey. On average, a year of pembrolizumab or atezolizumab can run between $50,000 and $150,000 in the United States, depending on dosage, insurance coverage, and infusion center fees.
Financial assistance
Many drug manufacturers offer copay assistance or patientsupport programs. For example, Mercks KeytrudaAssist program and Genentechs TruqAid can offset outofpocket costs for eligible patients. The resource page also lists charities that help navigate insurance gaps.
Is immunotherapy covered for all stages?
Not exactly. Coverage is typically granted when:
- The tumor is triplenegative and expresses PDL1 1% (for atezolizumab).
- Highrisk earlystage disease meets clinicaltrialderived criteria (e.g., 10% tumorinfiltrating lymphocytes).
- Hormonepositive disease is being studied in combination trials standard insurance usually does not pay for that yet.
For estrogenpositive breast cancer, a 2022 exploratory study showed only modest benefits when pembrolizumab was paired with endocrine therapy, and insurers remain hesitant ().
Treatment logistics
Most checkpoint inhibitors are given as an intravenous infusion every three weeks, lasting 3060minutes. Some centers offer homeinfusion services, which can reduce travel time and the emotional toll of weekly trips.
Before starting, its wise to prepare a simple checklist:
- Current medication list (including overthecounter supplements).
- Recent blood work results.
- Contact information for a trusted family member or friend to accompany you.
- Insurance preauthorization details.
Bottom Line
Immunotherapy isnt a miracle cure, but for the right breastcancer subtype especially triplenegative disease it offers a measurable boost in survival and a chance for a deeper, more durable response. The tradeoff is a distinct sideeffect profile and a hefty price tag, making open communication with your oncology team essential.
Ask your doctor about PDL1 testing, clinicaltrial eligibility, and financialassistance options. If youre curious or have personal stories to share, drop a comment below were all in this together, and your experience could help someone else decide whats best for them.
For related information on treatment outcomes and life expectancy after prostate procedures, see prostate removal life expectancy which discusses survival considerations that some patients weigh when choosing major cancer treatments.
FAQs
Is immunotherapy effective for early‑stage breast cancer?
In early‑stage triple‑negative breast cancer, adding immunotherapy to chemotherapy raises pathologic complete response rates from about 51 % to 64 %.
What are the most common immune‑related side effects?
Typical side effects include fatigue, skin rash, colitis, thyroiditis, and pneumonitis; severe (grade 3‑4) events occur in roughly 10‑15 % of patients.
Do I need PD‑L1 testing before starting immunotherapy?
Yes—PD‑L1 expression (≥1 % for atezolizumab) helps determine eligibility, especially for metastatic triple‑negative disease.
How much does a year of pembrolizumab or atezolizumab usually cost?
U.S. pricing ranges from $50,000 to $150,000 per year, though manufacturer assistance programs and insurance can reduce out‑of‑pocket expenses.
Can immunotherapy be combined with hormone therapy for ER‑positive cancers?
Current data show modest benefit; most insurers do not cover this combination outside clinical trials.