Imagine eating normally and still watching the scale climb faster than a rollercoaster. For many people with damage to the hypothalamus, that's everyday reality. The good news? There are real, science-backed ways to take back control of hunger, weight, and wellbeing. Below, I'll walk you through what hypothalamic obesity is, why it's different, andmost importantlywhat you can actually do about it.
Understanding Hypothalamic Obesity
What causes hypothalamic obesity?
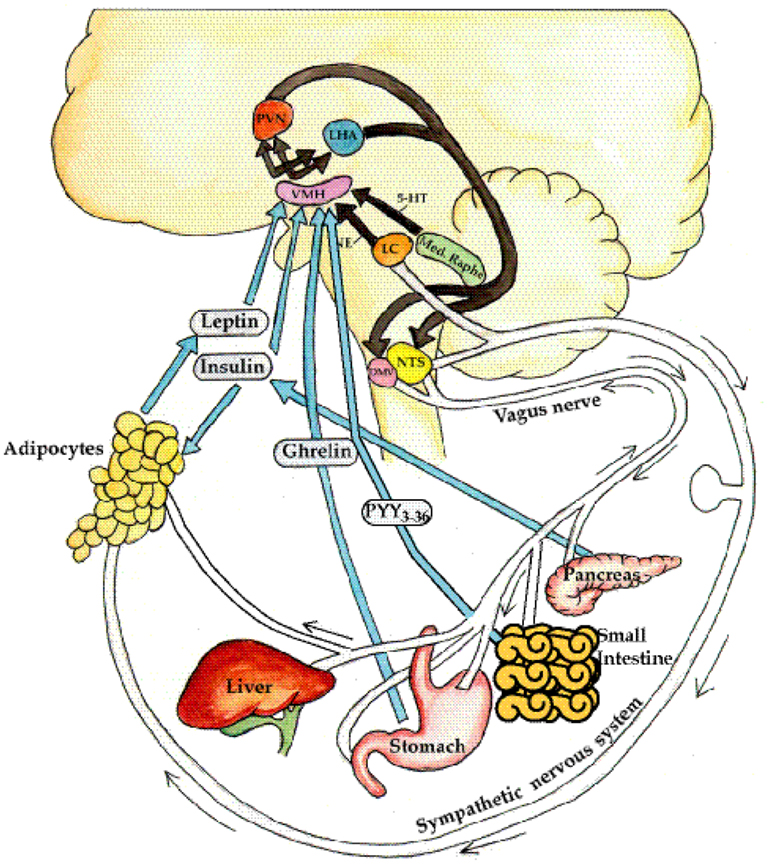
The hypothalamus is the brain's command center for appetite, metabolism, and hormone balance. When it gets hurtby a tumor, surgery, radiation, traumatic brain injury, or rare genetic syndromesits signals go haywire. This disruption is what we callhypothalamic obesity causes. The result? A relentless drive to eat, even when the stomach is technically full. Some of these hormonal imbalances can also be linked to other conditions, such as primary hypothyroidism, which affects thyroid hormone levels.
How common is hypothalamic obesity?
While it's still considered a rare condition, studies show it affects up to 5% of patients after craniopharyngioma surgery and a notable portion of those with pituitary disorders. In plain terms, if you know ten people who've undergone brain tumor treatment, one of them might be wrestling with this weight-gain challenge.
Which symptoms signal hypothalamic obesity?
- Rapid, unexplained weight gain (often 5-10kg in weeks)
- Persistent, intense hunger (hyperphagia)
- Fatigue despite adequate sleep
- Hormonal deficiencies (thyroid, cortisol, growth hormone)
- Emotional swings or depression linked to body image
How is it diagnosed?
Diagnosing hypothalamic obesity starts with a careful clinical history and physical exam. Doctors then order MRI scans to visualize hypothalamic injury and a panel of endocrine labs to check hormone levels, including checking for symptoms of low thyroid hormone levels. According to the latest research, a definitive diagnosis hinges on ruling out other causes of weight gain and confirming hypothalamic dysfunction.
Diagnostic Flowchart
| Step | What to Do |
|---|---|
| 1. Clinical Signs | Rapid weight gain + hyperphagia |
| 2. Hormone Panel | Check cortisol, thyroid, GH, sex steroids |
| 3. Imaging | Brain MRI focusing on hypothalamus |
| 4. Specialist Referral | Endocrinologist or neurooncology team |
Why Treatment Differs
What makes weight loss harder in hypothalamic obesity?
The damaged hypothalamus often leads to leptin resistance (the hormone that tells us we're full) and a slower resting metabolic rate. In plain language, your body acts like it's stuck on "eat more, burn less" mode, making diet-only approaches far less effective than they are for regular obesity.
FAQs
What is the primary cause of hypothalamic obesity?
Damage to the hypothalamus from tumors, surgery, radiation, injury, or genetic syndromes disrupts appetite and metabolism regulation, leading to uncontrolled weight gain.
Can medications really help control hunger in hypothalamic obesity?
Yes. GLP‑1 receptor agonists (e.g., semaglutide) and emerging drugs like setmelanotide target brain pathways that reduce appetite and promote weight loss.
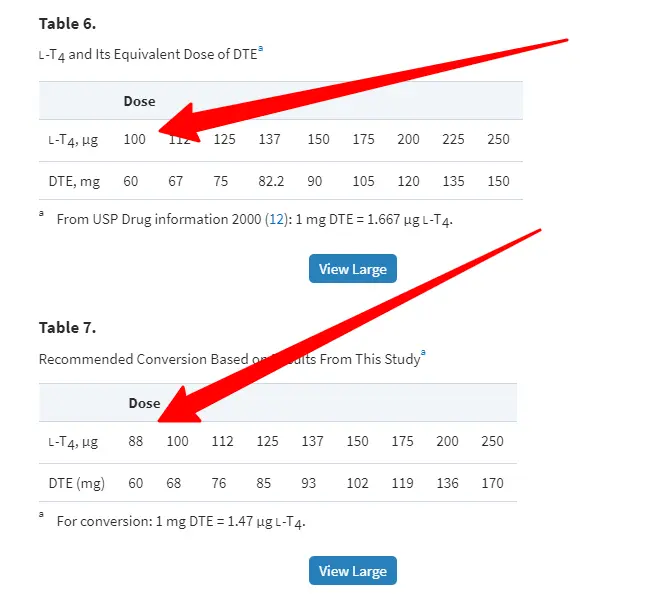
How does hormone replacement affect weight management?
Restoring deficient pituitary hormones (thyroid, cortisol, growth hormone, sex steroids) can boost metabolism and improve the effectiveness of diet and exercise plans.
Is bariatric surgery a viable option for hypothalamic obesity?
Surgery may be considered for severe cases, but because the hypothalamic drive to eat often persists, comprehensive medical and lifestyle support is still required.
What lifestyle changes are most important for adults with this condition?
High‑protein, low‑glycemic meals, regular moderate‑intensity cardio, strength training, and behavioral therapy together provide the best chance for sustainable weight loss.