You feel a small lump in your neck it looks harmless, but could it be a thyroid nodule? Most thyroid nodules are benign and cause no problems, yet a tiny% can be cancerous or affect hormone balance. Knowing the signs, when to get checked, and what treatment options exist saves anxiety and guides proper care.
What Is a Nodule
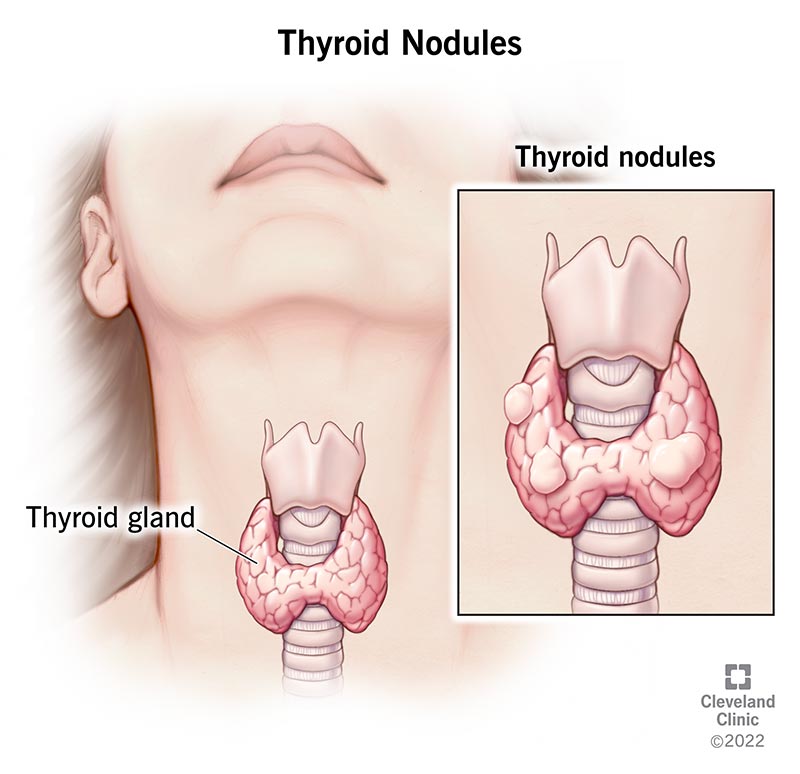
A thyroid nodule is simply an abnormal growth of cells within the thyroid gland, the little butterflyshaped organ at the base of your throat. The growth can be solid, fluidfilled (cystic), or a mix of both, and it may talk to you in different ways sometimes youll feel a palpable lump, other times an ultrasound will spot it incidentally.
Types of Nodules
- Solid vs. cystic: Solid nodules are made of dense thyroid tissue, while cystic ones are filled with fluid and often feel softer.
- Hot vs. cold: Hot nodules produce excess thyroid hormone and show up bright on a radioactive iodine scan; cold nodules are less active and, statistically, a bit more suspicious for cancer.
How Common Are They?
| Group | Prevalence |
|---|---|
| General adult population | 50% have at least one nodule on ultrasound |
| Women (especially 4565) | Higher up to 70% in some studies |
| Malignant nodules | About 515% of detected nodules |
Women tend to develop thyroid nodules more often than men, which is why you'll see the phrase woman thyroid nodules: symptoms pop up in many searches. This higher prevalence is also notable in conditions such as primary hypothyroidism, where women account for a majority of cases, often due to underlying autoimmune disorders.
Why Do They Form?
Most nodules arise spontaneously a glitch in cell growth that most of the time stays harmless. Iodine deficiency, inflammation (thyroiditis), or a family history of thyroid disease can also play a role. If you've ever wondered is a 2.5cm thyroid nodule large?, the answer depends on the context size alone isn't a verdict, but it does steer the next steps.
Symptoms and Warning Signs
Imagine you're scrolling through Instagram and a friend posts a photo of a swollen neck. You pause. Is that a thyroid nodule? you think. The reality is, many nodules stay quiet for years. Here's what to watch for:
Common, Usually Benign Symptoms
- A palpable lump in the front of your neck that moves when you swallow.
- Occasional mild discomfort or a feeling of tightness.
- No change in voice, swallowing, or breathing.
RedFlag Signs That Warrant a Doctors Visit
- Rapid growth of the lump.
- Hoarseness or voice changes.
- Difficulty swallowing or breathing.
- Persistent pain in the neck or ear.
- Unexplained weight loss, night sweats, or persistent fatigue.
These are the very questions behind what are the symptoms of cancerous thyroid nodules? they tend to involve pressure on nearby structures or systemic signs of thyroid hormone imbalance. If you experience symptoms suggestive of thyroid dysfunction, such as unexplained fatigue, hair loss, or menstrual changes, it's helpful to read about the hypothyroidism effects that can overlap with nodule symptoms.
Size Matters: Is a 2.5cm Nodule Large?
In plain language, a 2.5cm nodule is about the size of a small grape. It's not huge, but it's big enough that most clinicians will suggest further imaging or a fineneedle aspiration (FNA) biopsy, especially if it's solid and has suspicious features on ultrasound.
When Blood Tests Are Normal
It's not unusual to see thyroid nodules but blood tests normal as a search query. A normal TSH, T3, and T4 level simply means the nodule isn't overproducing hormones. However, normal labs do not rule out structural concerns, so imaging still matters. Sometimes, nodules are found in the context of overall thyroid hormone deficiencyand your doctor will use your clinical picture and imaging features to guide next steps.
Diagnosis Steps Explained
If you've booked an appointment, the doctors roadmap is usually straightforward: feel, see, and (if needed) sample. Here's the typical flow.
Physical Examination
The doctor will gently press on the front of your neck while you swallow. A nodule that moves with swallowing is a classic sign that it's attached to the thyroid.
Imaging The Ultrasound Star
Highresolution ultrasound is the gold standard. It shows the nodule's size, composition, margins, calcifications, and blood flow. A study in the National Institutes of Health found that ultrasound alone can correctly classify benign versus suspicious nodules in about 80% of cases.
Key Ultrasound Features to Note
| Feature | Benign Indicator | Suspicious Indicator |
|---|---|---|
| Echogenicity | Iso or hyperechoic | Hypoechoic |
| Margins | Smooth, welldefined | Irregular, microlobulated |
| Calcifications | None or macrocalcifications | Microcalcifications |
| Vascularity | Peripheral | Central |
FineNeedle Aspiration (FNA) Biopsy
If the nodule is larger than 1cm and has any suspicious ultrasound pattern, the endocrinologist will likely recommend an FNA. A thin needle extracts a few cells, which a cytopathologist examines under a microscope.
According to the , the Bethesda System categorizes results from benign to malignant, guiding whether surgery is needed.
Molecular Testing (Optional)
In ambiguous cases, doctors may send the FNA sample for genetic markers (e.g., BRAF, RAS). These tests help refine the cancer risk estimate, especially when the cytology falls into the indeterminate category.
Treatment Options Overview
Here's where the conversation shifts from what is it? to what now? The good news is that the majority of nodules never require invasive treatment.
Active Surveillance The WatchandWait Approach
If the nodule is small, stable, and benign on biopsy, many physicians suggest monitoring it with periodic ultrasounds every 612months. This strategy avoids unnecessary surgery and its associated risks.
Typical FollowUp Timeline
- 0months Baseline ultrasound.
- 6months Repeat imaging to confirm stability.
- 12months If unchanged, shift to annual scans.
Medication: Levothyroxine Suppression
Some endocrinologists prescribe lowdose levothyroxine to slightly suppress TSH, hoping to shrink the nodule over time. Recent metaanalysis (2023) suggests modest size reduction in a subset of patients, but the evidence isn't strong enough to make it a universal recommendation. Understanding your low thyroid hormone status and discussing options with your endocrinologist can help clarify if this approach may be appropriate for you.
Radioactive Iodine (RAI) Therapy
RAI is mainly used for nodules that produce excess hormone (hot nodules) or for certain lowrisk cancers. It works by delivering targeted radiation that destroys thyroid tissue while sparing most of the surrounding neck structures.
Pros & Cons of RAI
| Pros | Cons |
|---|---|
| Nonsurgical, outpatient | Potential temporary dry mouth, taste changes |
| Can treat multifocal disease | Requires radiation safety precautions |
Surgical Options When Removal Is Needed
If the nodule is malignant, rapidly growing, or causing compressive symptoms, surgery is the definitive solution. The two main procedures are:
- Lobectomy: Removal of the affected thyroid lobe. Usually enough for small, localized cancers.
- Total thyroidectomy: Entire gland removal. Reserved for larger cancers or bilateral nodules.
Postop care includes calcium monitoring (to avoid hypocalcemia) and lifelong thyroid hormone replacement if the whole gland is taken out.
Emerging Minimally Invasive Techniques
Thermal ablation (radiofrequency or microwave) and ethanol injection are gaining traction for patients who want to avoid surgery. Early trials show promising nodule shrinkage with minimal downtime, but longterm data are still being gathered.
Balancing Benefits & Risks
Deciding on a path forward can feel like standing at a crossroads. On one side, early detection offers peace of mind and the chance to treat a cancer before it spreads. On the other, overtreatment can bring surgical complications, unnecessary radiation exposure, and a lot of stress.
Pros of Early Action
- Potential to catch a malignancy at a curable stage.
- Better control over symptoms like throat pressure or hormone imbalances.
- Reduced anxiety once you have a clear plan.
Cons of Overtreatment
- Risk of vocal cord injury, hypoparathyroidism, or scar tissue after surgery.
- Possible sideeffects from radioactive iodine (dry mouth, temporary taste loss).
- Emotional toll of unnecessary medical procedures.
Shared DecisionMaking Tips
Ask your doctor about the exact risk each finding represents. Request a copy of the ultrasound images and the biopsy report. If something feels off, get a second opinion it's your body, and you deserve clarity.
Quick Checklist for Your Next Visit
- Bring a list of symptoms (even the subtle ones).
- Know your family history of thyroid or other endocrine disorders.
- Ask about the need for FNA based on nodule size and ultrasound features.
- Discuss the pros and cons of active surveillance versus immediate treatment.
- Request reputable sources or guidelines (e.g., ATA 2023 guidelines) to review later.
Conclusion
Thyroid nodules are common, and most of them are harmless. Still, a small percentage can signal something more serious, so staying informed about symptoms, diagnostic steps, and treatment avenues is essential. By understanding what to look for, how doctors evaluate a nodule, and the spectrum of management options, you can make confident, shared decisions with your healthcare team. If you've felt a lump, don't waitschedule a checkup, ask questions, and consider downloading a trusted guide to keep your thyroid health on track.
FAQs
What exactly is a thyroid nodule?
A thyroid nodule is an abnormal growth of cells within the thyroid gland that can be solid, cystic, or a mix of both.
How can I tell if a thyroid nodule is dangerous?
Dangerous nodules often show suspicious features on ultrasound (e.g., microcalcifications, irregular margins) or cause rapid growth, voice changes, or hormone imbalances.
When is a fine‑needle aspiration (FNA) biopsy needed?
FNA is usually recommended for nodules larger than 1 cm with concerning ultrasound characteristics or any size if the cytology is unclear.
Can a thyroid nodule be treated without surgery?
Yes. Options include active surveillance, low‑dose levothyroxine suppression, radioactive iodine for hot nodules, and minimally invasive ablative therapies.
What follow‑up schedule is typical for a benign thyroid nodule?
After an initial baseline ultrasound, most doctors repeat imaging at 6 months, then annually if the nodule remains stable.