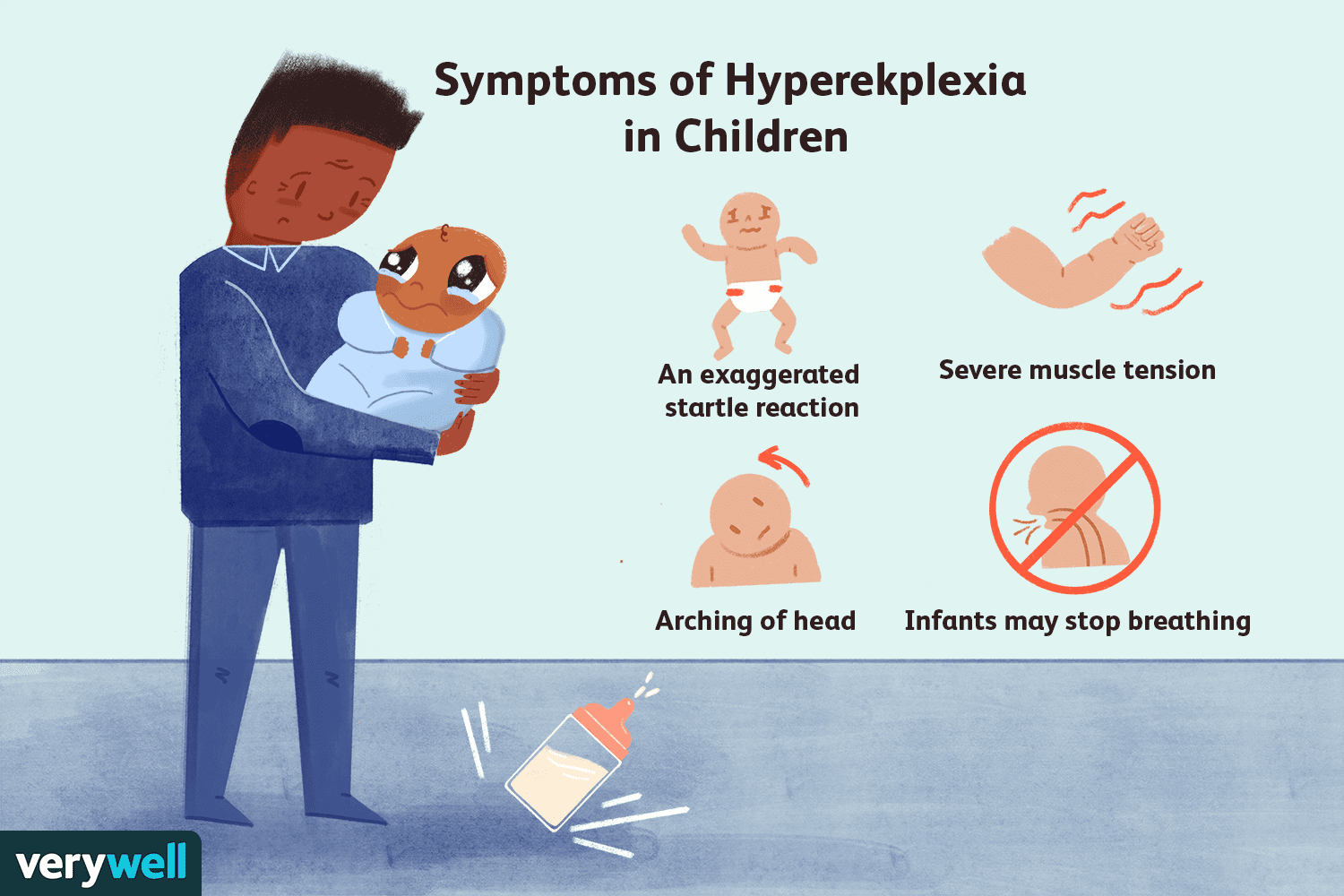
At first, I thought it was nothing You know that moment when a baby suddenly stiffens or an adult jumps at the slightest sound, and you brush it off as just a reflex? In many cases that quick startle is harmless, but for some its a clue that something called hyperekplexia is at play. Spotting the three hallmark signsbirthtime stiffness, an exaggerated startle, and a brief poststartle rigiditylets doctors confirm the diagnosis early, avoid costly misdiagnoses, and start the right treatment.
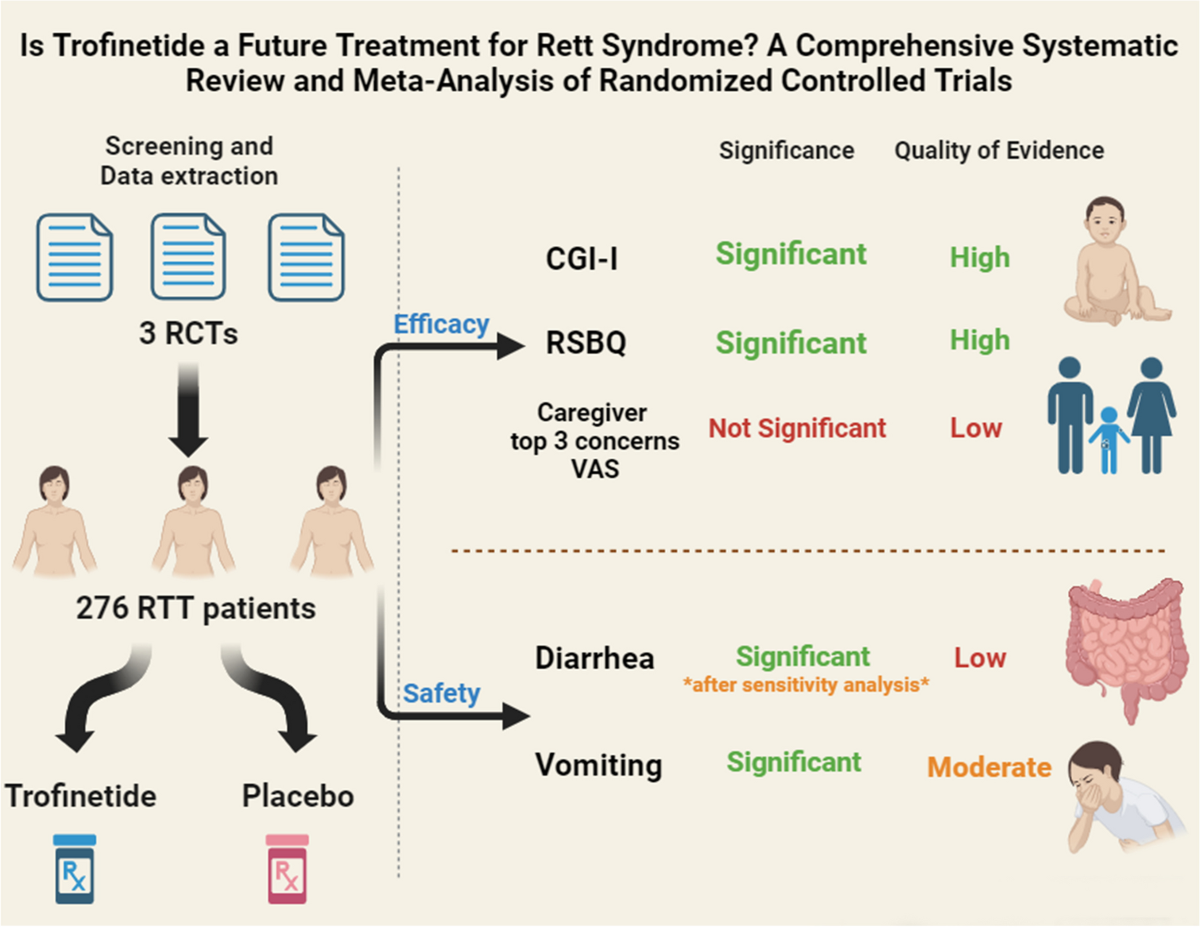
Getting the right hyperekplexia diagnosis can feel like finding a missing puzzle piece. It turns uncertainty into a clear plan, and it can make the difference between living with frequent scares and managing a condition thats actually treatable. Lets walk through what hyperekplexia is, how its diagnosed, and what you can do nexttogether. For families navigating rare neurological conditions, resources on atypical Rett syndrome can also offer helpful context about genetic testing and specialist referrals.
What Is Hyperekplexia
Hyperekplexia, sometimes nicknamed startle disease, is a rare neurological disorder that amplifies the bodys startle reflex. It can show up the moment a baby is born or later in life, and its usually inherited through genes that affect the glycine pathway in the spinal cord. While only a handful of families worldwide are affected, the impact on daily life can be huge if the condition goes unnoticed.
Who Can It Affect?
Most cases are diagnosed in newborns, but does occur. Adults may have a milder form that only becomes noticeable after a sudden loud noise or a minor bump. The condition doesnt discriminatemen, women, and children can all experience it.
Is It Dangerous?
The disorder itself isnt lifethreatening, but the exaggerated startle can lead to injuriesthink falling off a chair or hitting your head after a sudden jerk. Misdiagnosis, especially as epilepsy, can also delay proper treatment, which is why a precise hyperekplexia diagnosis matters.
QuickFacts Comparison
| Feature | Hyperekplexia | Epilepsy | Cerebral Palsy |
|---|---|---|---|
| Startle trigger | Any sudden sound/touch | Specific seizure focus | Usually constant tone |
| EEG result | Normal | Abnormal spikes | Usually normal |
| Postevent rigidity | Secondsminutes | Variable, often longer | Not typical |
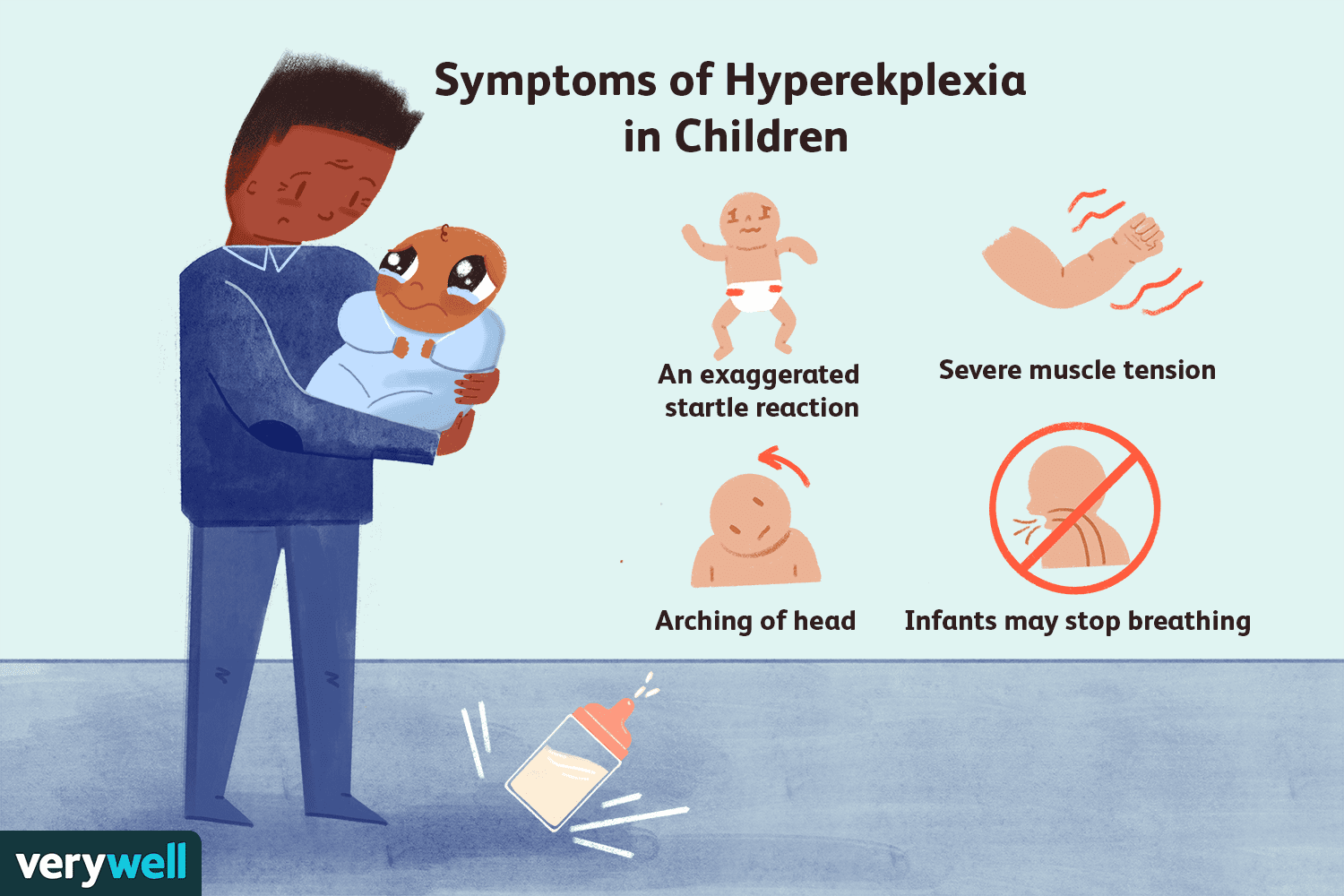
Diagnostic Triad
Doctors rely on a classic triad to pinpoint hyperekplexia. When all three appear, the suspicion becomes very strong.
1. Generalized Stiffness at Birth
This isnt the usual newborn flexed posture. Babies with hyperekplexia often appear unusually rigid, with limbs held in a tight, extended position. Parents may describe the infant as stonecold straight after delivery.
2. Exaggerated Startle Response
Even a gentle tap on the nose or a soft clap can send a childor an adultinto a fullbody jerk. The reaction is far beyond what youd expect from a normal reflex.
3. Brief PostStartle Rigidity
After the startle, the body freezes for a few seconds to a couple of minutes. Its that moment when you see someone hanging midjump, eyes wide, muscles locked.
The NoseTap Test (Glabella Tap)
Clinicians often perform a gentle tap on the glabella (the smooth area between the eyebrows). A positive result is an immediate, vigorous jump followed by a short rigidity phase. The test is safe, quick, and highly indicative when interpreted alongside the other two signs.
Differential Diagnosis
Because hyperekplexia mimics other conditions, doctors must rule out a few lookalikes.
Epilepsy vs. Hyperekplexia
Both can present with sudden jerks, but an EEG (electroencephalogram) will show epileptic spikes in seizures, while it remains normal in hyperekplexia. The startleinduced rigidity also resolves much faster in hyperekplexia.
Other Mimics
Neonatal seizures, cerebral palsy, and even anxietyrelated hyperreactivity can cause startling behaviours. A thorough historyespecially noting the threepoint triadhelps separate these.
DecisionTree Flowchart
| Step | What to Look For | Next Action |
|---|---|---|
| 1. Birth history | Rigidity at delivery? | Proceed to startle test |
| 2. Startle test | Exaggerated jump + brief rigidity? | Order genetic panel |
| 3. EEG | Normal? | Supports hyperekplexia |
Diagnostic Process
StepbyStep Guide for Families
- Collect the story: Write down when the stiffness first appeared, any triggers, and family members with similar symptoms.
- Physical exam: A pediatric neurologist (or neurologist for adults) will perform the nosetap and observe the response.
- Genetic testing: Panels target genes like GLRA1, SLC6A5, and others involved in the glycine pathway. A positive result clinches the diagnosis.
- Electrophysiology (optional): EMG can show abnormal muscle activity during the startle, while EEG helps rule out seizures.
- Review results together: Your doctor should explain the findings in plain language, outline treatment, and answer any whatif questions you have.
Sample Report Template
| Section | Details |
|---|---|
| Clinical History | Birth stiffness, startle triggers, family pedigree |
| Physical Exam | Positive nosetap, 3point triad present |
| Genetics | GLRA1 mutation detected |
| EEG/EMG | Normal EEG; EMG shows brief hyperactivity |
| Conclusion | Confirmed hyperekplexia diagnosis |
Treatment Options
Even though the articles focus is diagnosis, youll likely wonder, What happens after the label? The good news: several effective strategies exist.
FirstLine Medications
Clonazepam is often the goto drug; it dampens the overactive startle reflex. Baclofen may be added for muscle tone control. Doses start low and are titrated under a physicians watchful eye.
NonPharmacologic Strategies
- Physical therapy: Helps children develop safe movement patterns and reduces injury risk.
- Environment tweaks: Soft furnishings, cushioned corners, and clear pathways can prevent falls during a startle.
- Startlereduction training: Gradual exposure to mild stimuli can desensitize the reflex over time.
LongTerm Outlook & Lifespan
With early diagnosis and proper treatment, most people lead full lives. Studies show that untreated hyperekplexia can lead to recurrent injuries and psychosocial stress, while treated individuals often experience a marked reduction in startling episodes and enjoy a normal . The condition itself isnt fatal, but the secondary effects can be serious if ignored.
CaseStudy Box
| Age at Diagnosis | Intervention | Outcome (5year followup) |
|---|---|---|
| 3months | Clonazepam+physio | 90% reduction in startle frequency; normal developmental milestones. |
| 28years | Lowdose clonazepam | Improved work safety; minimal sideeffects. |
Resources & Support
Finding reliable information and a community that gets it can turn anxiety into empowerment.
Trusted Medical Organizations
- detailed clinical overview.
- patient resources.
- global raredisease database.
Patient & Family Networks
Online forums, Facebook groups, and local raredisease meetups let families share tipslike the best brand of softcorner protectors or how to talk to a school about startle safety.
When to Seek a Second Opinion
If you feel the diagnosis was rushed, or the treatment isnt easing the startle, its perfectly reasonable to ask for a referral to a pediatric (or adult) neurologist who specializes in rare movement disorders. Bring the triad checklist and any genetic reports to make the consultation smoother. For help navigating insurance and access to therapies, some families find information about Exondys 51 insurance processes useful as a model for working with payers and specialty medication approvals.
Referral Letter Checklist
| Item | Details to Include |
|---|---|
| Patient history | Birth stiffness, startle incidents, family cases |
| Physical findings | Results of nosetap test, duration of rigidity |
| Test results | Genetic panel, EEG/EMG reports |
| Current meds | Dosages, sideeffects, response |
Conclusion
Getting a clear hyperekplexia diagnosis is more than a labelits a roadmap. By recognizing the three hallmark signs, confirming them with a simple nosetap test and genetic analysis, and partnering with knowledgeable clinicians, families can move from uncertainty to a proactive care plan. Early treatment dramatically lowers the risk of injury, improves quality of life, and opens the door to a supportive community.
If youve noticed unusual startle reactions in yourself or a loved one, dont wait. Talk to your doctor, ask about the diagnostic triad, and explore the options that can help you live with confidence. Have you or someone you know navigated a hyperekplexia diagnosis? Share your story in the commentsyour experience could be the clue that helps another family feel seen and hopeful.
FAQs
What are the three main signs doctors look for in a hyperekplexia diagnosis?
The classic triad includes generalized stiffness at birth, an exaggerated startle response to minor stimuli, and a brief period of post‑startle rigidity lasting seconds to minutes.
How is the nose‑tap (glabella tap) test performed?
A clinician gently taps the glabella—the smooth area between the eyebrows. A positive result is an immediate, vigorous jump followed by short rigidity, indicating a hyper‑reactive startle reflex.
Can an EEG help differentiate hyperekplexia from epilepsy?
Yes. In hyperekplexia the EEG is typically normal, whereas epilepsy shows characteristic abnormal spikes or waveforms during seizures.
Which genetic mutations are most commonly associated with hyperekplexia?
Mutations in the GLRA1, SLC6A5, and other genes affecting the glycine inhibitory pathway are the most frequently identified causes.
What treatment options are available after confirming a hyperekplexia diagnosis?
First‑line medication such as clonazepam (often combined with baclofen) can reduce startle intensity. Physical therapy, environmental safety modifications, and gradual desensitization training are also important components of management.