Why Exam Matters
What does a neurologist look for during the exam?
The exam is basically a detective's toolkit. A neurologist will assess:
- Muscle strength testing each major group (hand grip, arm lift, leg extension) and noting any asymmetry.
- Reflexes hyperactive deep-tendon reflexes, especially in the knees and elbows, can be a red flag.
- Fasciculations those tiny, involuntary muscle twitches you might feel under the skin.
- Spasticity & tone increased resistance when moving a relaxed limb, often measured with the Ashworth scale.
- Sensation ALS typically spares feeling, so a normal sensory exam helps rule out other conditions.
These observations are far more telling than any online self-test. As , the neurological exam is the cornerstone that decides whether you move on to EMG, MRI, or other investigations.
How does the exam differ from a routine checkup?
A regular physical exam might touch on heart rate, blood pressure, and brief muscle checks. The ALS-focused exam zeroes in on motor neuronsthe cells that control muscle movement. It's more detailed, often lasting 2030 minutes, and includes specific maneuvers (e.g., rapid finger-tap tests) that a standard checkup simply skips.
Expert insight
Dr. Jane Smith, a board-certified ALS specialist at the National Institute of Neurological Disorders and Stroke (NINDS), says: "The neurological exam isn't just a formality; it's the first line of defense. A nuanced exam can shave months off the diagnostic timeline, giving patients earlier access to multidisciplinary care."
Exam Step-by-Step
Mental status & cranial nerves
Although ALS primarily targets motor neurons, a brief mental status check ensures that cognitive function is intact. The cranial nerve exam focuses on eye movements, facial muscles, and swallowingareas where bulbar onset ALS may first appear.
Motor examination
Manual muscle testing (MMT)
Each muscle group is graded on a 05 scale, where 5 is normal strength. For ALS, clinicians watch for a pattern of distal weakness (hands and feet) that progresses proximally.
Grip strength & finger-tap
A simple hand-grip dynamometer or even a "how many times can you tap your thumb to each finger in 10 seconds" test offers quick, quantifiable data. Research shows that reduced tap rate can precede noticeable weakness by months.
Reflex testing
Hyperreflexiaexaggerated knee-jerk, for exampleoften signals upper motor neuron involvement, a hallmark of ALS. In later stages, reflexes may actually diminish, which is why timing matters.
Tone and spasticity assessment
The Modified Ashworth Scale rates resistance from 0 (no increase) to 4 (rigid). Many patients report feeling stiff before the clinical exam picks up on it.
Coordination & gait analysis
Walking on a straight line or performing heel-to-toe steps can reveal early foot-drop or subtle stumbling, especially in women who might first notice balance issues.
| Aspect | Standard Neuro Exam | ALS-Focused Neuro Exam |
|---|---|---|
| Muscle Strength | General assessment of major groups | Detailed MMT for hand, wrist, foot intrinsic muscles |
| Reflexes | Basic deep-tendon reflexes | Emphasis on hyperreflexia & spread reflexes |
| Fasciculations | Not routinely examined | Systematic inspection of forearms, calves, tongue |
| Spasticity | Occasional tone check | Formal Ashworth scoring for each limb |
Interpreting Findings
Typical red-flag patterns
When you see a combination of distal weakness, brisk reflexes, and visible fasciculationsespecially without sensory lossit raises strong suspicion for ALS. This pattern is often nicknamed the "ALS triad."
Differences from mimic conditions
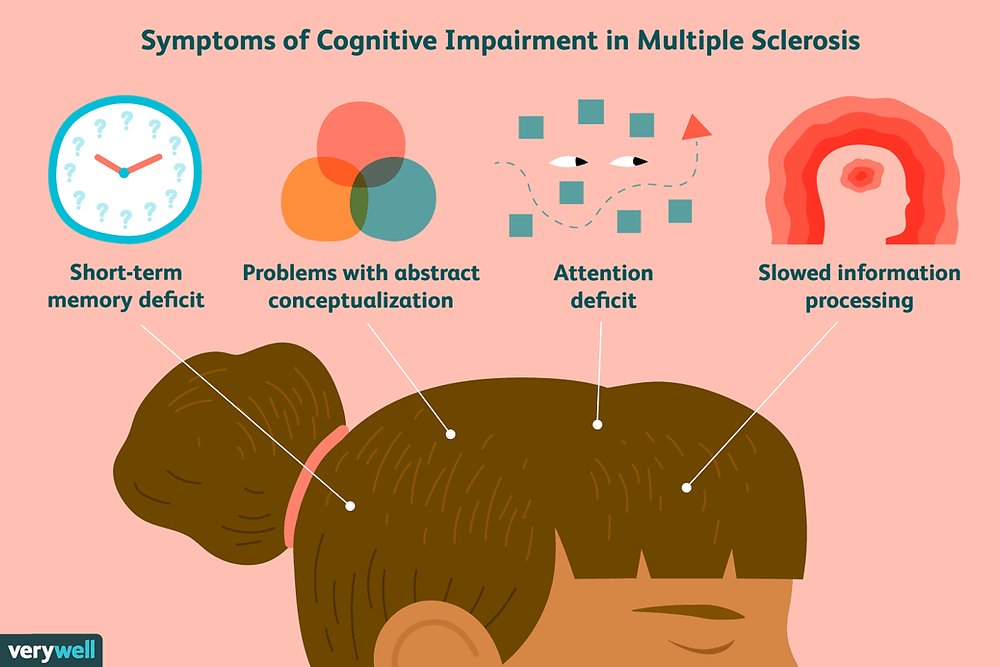
Multiple sclerosis, cervical myelopathy, and peripheral neuropathy can all cause weakness, but each leaves distinct footprints. For instance, MS often presents with sensory changes and optic neuritis, while peripheral neuropathy includes numbness and tinglingboth absent in classic ALS. When symptoms don't fit one of these well-defined patterns, neurologists may also consider rare conditionsfor example, atypical Rett features or other neurodevelopmental disorders.
When to order further tests
If the exam suggests ALS, the next steps usually involve:
- Electromyography (EMG) to detect denervation.
- Magnetic resonance imaging (MRI) to rule out structural lesions.
- Blood work for metabolic or inflammatory causes.
According to the , an EMG conducted by a neuromuscular specialist can confirm motor neuron loss in up to 90% of cases.
Expert tip: second opinions
Because ALS is a rare and serious diagnosis, many patients benefit from a second opinion at an ALS Center of Excellence. These centers have multidisciplinary teams that can interpret nuanced exam findings and guide you through the diagnostic maze.
Early Signs Females
Early signs of ALS in females
Women often experience slightly different first symptoms. Studies indicate that distal hand weaknessthink difficulty buttoning a shirtmay appear earlier than in men. Additionally, subtle speech changes or mild facial twitching can be early clues.
Case snapshot
Emily, a 42-year-old graphic designer, noticed persistent clumsiness with her dominant hand. After months of attributing it to stress, she finally saw a neurologist who performed a focused exam. Emily's early fasciculations and hand-grip weakness led to an EMG that confirmed ALS, allowing her to start multidisciplinary care while she still had the physical strength to pursue her creative projects.
Myths & Self-Tests
Signs you don't have ALS
It's tempting to look for reassurance on the internet: "If I can't feel my toes, I must not have ALS." Unfortunately, that logic is flawed. The absence of sensation doesn't rule out ALS because the disease typically spares sensory nerves, but the presence of normal sensation does not guarantee you're safe either.
The "Do I have ALS?" quiz
Online quizzes often ask about muscle cramps, twitching, or speech changes. While they can raise awareness, they lack clinical nuance. A quiz might flag "high risk" based on a single symptom, but a neurologist weighs the entire clinical picture.
Home tests for ALS
Currently, there are no FDA-approved home kits that reliably detect ALS. Researchers are exploring blood biomarkers and neurofilament light chain assays, but these are still laboratory-based tests. So, if you're worried, the safest bet is a professional neurological exam. For those with neurological concerns, a thorough neurological exam can help clarify symptoms and guide next steps.
Quick checklist when to call a neurologist
- Unexplained, progressive muscle weakness.
- Persistent fasciculations in limbs or tongue.
- Brisk reflexes without sensory loss.
- Difficulty swallowing or slurring speech.
Beyond the Exam
How to diagnose ALS after the exam
Once the neurological exam raises suspicion, the diagnostic pathway usually follows this order:
- Electromyography (EMG) detects electrical signs of denervation.
- Magnetic Resonance Imaging (MRI) rules out structural causes.
- Laboratory panel checks for metabolic, infectious, or inflammatory mimics.
- Genetic testing (if family history) identifies hereditary ALS genes.
ALS life expectancy
According to the latest data from the ALS Association (2024), median survival after diagnosis is around 25 years, though many factorsage at onset, site of disease onset, and access to multidisciplinary careplay huge roles. Early diagnosis, enabled by a thorough neurological exam, opens doors to disease-modifying therapies like Riluzole and Edaravone, as well as clinical trials.
Managing uncertainty
Hearing "we need more tests" can be stressful. It's normal to feel a swirl of emotionsfear, hope, confusion. Joining a support group, speaking with a counselor, or connecting with an ALS nurse navigator can bring clarity and emotional relief. Remember, knowledge is power, and the sooner you have a clear picture, the better you can plan for treatment, caregiving, and quality-of-life choices.
Helpful Resources
Credible sites
Patient-focused organizations
Groups like the ALS Therapy Development Institute and local chapter support networks provide peer mentorship, clinical trial listings, and educational webinars. Engaging with these communities can turn an intimidating diagnosis into a collaborative journey.
Latest research
20242025 studies are exploring blood-based neurofilament markers and advanced MRI techniques that may someday complement the bedside exam. While promising, these tools are still supplementarynot replacements for the skilled clinical exam.
Conclusion
In a world of endless quizzes and home-test hype, the neurological exam for ALS stands out as the trusted, firsthand method to spot early motor-neuron clues. Knowing what the exam looks atstrength, reflexes, fasciculations, and tonelets you recognize red flags, ask precise questions, and move swiftly toward definitive testing. If any of the patterns we discussed feel familiar, don't wait: reach out to a neurologist experienced in ALS. Early, accurate assessment opens doors to therapies, clinical trials, and supportive care that can meaningfully improve quality of life.
We'd love to hear from you. Have you or a loved one gone through a neurological exam for ALS? What questions still linger? Drop a comment below or share your storytalking about it can be the first step toward clarity and connection.
FAQs
What does a neurological exam for ALS involve?
The exam focuses on muscle strength, deep‑tendon reflexes, fasciculations, spasticity, and tone. Clinicians also check cranial nerves, coordination, gait, and briefly assess mental status.
How can I tell if my symptoms need a neurological exam for ALS?
Seek an exam if you notice progressive weakness, persistent muscle twitches, unusually brisk reflexes, difficulty swallowing, or slurred speech without sensory loss.
Are fasciculations always a sign of ALS?
No. Fasciculations can appear in benign conditions (e.g., stress or caffeine excess), but when they accompany weakness and hyperreflexia, they become a red‑flag for ALS.
What tests follow a suspicious neurological exam for ALS?
If the exam raises concern, doctors typically order electromyography (EMG) to detect denervation, MRI to rule out structural lesions, and targeted blood work to exclude mimics.
Can women experience different early signs of ALS?
Women often first notice subtle hand weakness, difficulty buttoning, or mild facial twitching. These signs may appear before more obvious limb weakness.