During a migraine workup the exam is usually pretty bland most of the time you'll find nothing abnormal. The real magic happens when you spot the red-flag clues that signal a more serious headache lurking underneath. Below you'll get the quick-check list, the warning signs you must never miss, and step-by-step tips on how clinicians actually perform the exam.
Why Exam Matters
What the exam aims to rule out
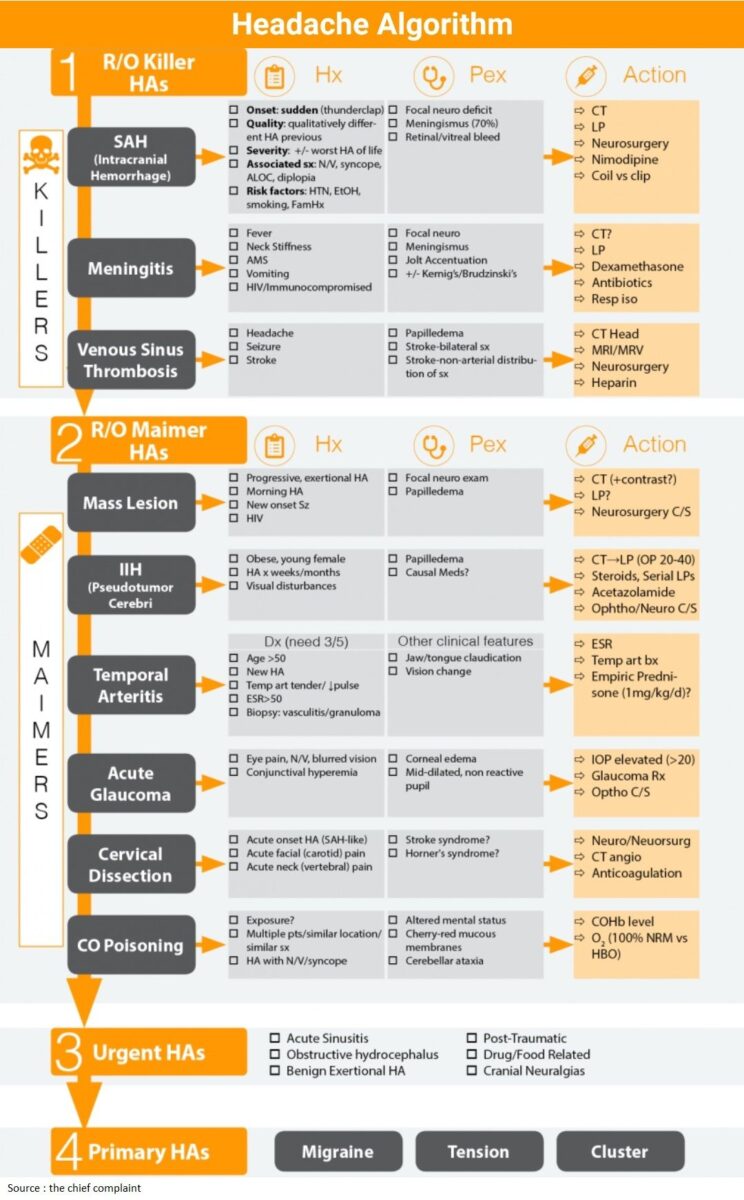
Even though migraines are defined mostly by the story you tell, doctors still need to make sure the story isn't hiding something dangerous. A thorough physical exam helps rule out conditions like subarachnoid hemorrhage, meningitis, temporal arteritis, or a brain tumor.
How neurologists and primary-care doctors differ
In a busy clinic a primary-care physician often runs a rapid OSCE-style checklist (think 5-minute quick screen). Neurologists, when time allows, can dive deeper adding a more detailed cranial nerve exam or extra neurovascular testing. Both approaches share the same goal: confirm a primary migraine and exclude secondary causes.
Quick-check OSCE table
| Step | What to do | Key finding |
|---|---|---|
| 1 | Vital signs | Fever>38C red flag |
| 2 | Scalp & sinus palpation | Tenderness sinusitis |
| 3 | Neck exam (flex/extend) | Stiff neck meningitis |
| 4 | Fundoscopy | Papilledema increased ICP |
| 5 | Neurologic screen (Cranial IIXII) | Focal deficit secondary cause |
Core Exam Findings
Typical (nonpathologic) findings
Most migraine patients walk out of the exam room with a completely normal neurological check. No fever, no papilledema, and no focal weakness. You might notice a bit of scalp tenderness or tight neck muscles that's the body's way of reacting to the pain, not a sign of something else.
Red-flag findings that must change your diagnosis
These are the deal-breakers. If any show up, the workup jumps from migraine to urgent imaging or labs.
- Systemic symptoms: fever, unexplained weight loss, night sweats (think infection or malignancy).
- Focal neurological signs: unilateral weakness, numbness, speech problems, or visual field cuts.
- Urgent ocular signs: papilledema or sudden visual loss.
- Temporal artery tenderness or jaw claudication: classic for giant-cell arteritis, especially in patients over 50 check ESR/CRP urgently.
- Sudden thunderclap onset: a headache that peaks in seconds never ignore this.
Red-flag cheat sheet
SENTR a quick mnemonic you can keep in your pocket:
- S Systemic (fever, malaise)
- E Eyes (papilledema, visual loss)
- N Neuro (focal deficit, seizures)
- T Temporal artery tenderness / jaw claudication
- R Recent sudden onset (thunderclap)
How to document findings for a migraine report (PDF template)
Having a readymade report template can save you minutes. The template usually includes sections for vitals, scalp/temporal assessment, neck exam, neurologic screen, and a red-flag checklist. Fill it out, print, and hand it to your clinician they'll thank you.
Exam Step-by-Step
Preparation & patient positioning
Start by explaining what you're doing. "I'm just going to check a few things to make sure everything looks normal, okay?" A relaxed patient gives you better cooperation and more reliable findings.
Head & scalp inspection
Look for asymmetry, lesions, or swelling. Lightly run your fingers over the temples a little tenderness is common, but sharp pain might point to temporal arteritis.
Temporal artery and jaw assessment
Gently press the temporal region while the patient opens and closes the mouth. Pain or a diminished pulse? That's a red flag you can't ignore.
Sinus & TMJ palpation
Press over the frontal sinuses and the maxillary area. If the patient winces, you might be dealing with sinusitis masquerading as a migraine.
Neck examination
Ask the patient to flex, extend, and rotate the neck slowly. Stiffness or pain with movement could indicate meningitis or a cervical strain that's aggravating the headache.
Neurologic screen (Cranial IIXII, motor, sensory, coordination)
Run through a rapid quick screen: vision (checking for double vision), pupil size, eye movements, facial symmetry, shoulder shrug (CN XI), tongue protrusion (CN XII). Then test strength in the arms and legs, and a quick finger-to-nose test for coordination.
Sample script for clinicians
"First, let's check how your eyes move together. Great. Now I'll tap lightly over the temples. All good there. Finally, could you lift each arm straight out for a few seconds?" Hearing the patient say "Sure, no problem" is a good sign you're on track.
Findings & Diagnosis
ICHD-3 criteria for migraine where the exam fits
The International Classification of Headache Disorders, 3rd edition (ICHD-3), places the majority of diagnostic weight on the patient's history. The physical exam's role is to ensure there are no red-flag features that would move you out of the primary migraine category.
How neurologists use the exam to decide on imaging
Think of the exam as a decision tree:
- If the exam is completely normal and the history matches migraine, most neurologists will forgo immediate imaging.
- If any red-flag sign pops up fever, papilledema, focal deficit, sudden onset they order a CT or MRI right away.
For example, when temporal artery tenderness or jaw claudication appears, clinicians often expedite inflammatory markers and further evaluation for giant-cell arteritis to avoid vision-threatening complications.
Frequently used PDFs and resources
When you need a quick reference, clinical report templates and diagnostic criteria PDFs from headache societies are useful to keep on hand.
Real-World Case Vignettes
Typical migraine patient Emily, 29 (no red flags)
Emily walks into the office with a throbbing, unilateral headache that worsens with bright light. Her vitals are 98.6F, blood pressure normal, and she reports no recent illness. The exam:
- Scalp tender over the left temple mild.
- Neck range of motion full, no stiffness.
- Fundoscopy: clear optic discs, no papilledema.
- Cranial nerves IIXII intact, strength 5/5 everywhere.
Because everything checks out, Emily's clinician follows the ICHD-3 criteria, confirms a migraine, and prescribes a triptan with lifestyle counseling. No imaging needed.
Red-flag scenario Mark, 55 (temporal arteritis signs)
Mark arrives with a new-onset, unilateral headache that's been getting worse over weeks. He mentions jaw pain when chewing and a low-grade fever. The exam reveals:
- Marked tenderness over the right temporal artery, pulse faint.
- Elevated temperature 38.2C.
- Mild visual blurring, fundoscopic exam shows early optic disc swelling.
These findings trigger immediate ESR/CRP labs and a high-dose corticosteroid regimen while awaiting a temporal artery biopsy. Mark's case illustrates why the physical exam can be the gatekeeper between a routine migraine and a life-threatening vasculitis. For clinicians seeking patient assistance programs or insurance guidance when high-cost therapies are needed for neurologic conditions, resources on Exondys 51 assistance may offer useful models for navigating benefits and support.
Lessons learned
- Never assume a headache in patients over 50 is just a migraine.
- Check the temporal arteries whenever jaw claudication or scalp tenderness appears.
- Fever + neck stiffness = meningitis until proven otherwise.
Final Summary & Actions
In a nutshell, migraine physical exam findings are often "nothing to see here," but that's exactly why the exam is crucial it helps you spot the red-flag clues that demand urgent attention. Keep this quick checklist handy:
- Vitals especially fever.
- Scalp & temporal artery tenderness.
- Neck stiffness.
- Fundoscopic view for papilledema.
- Basic neurologic screen for focal deficits.
If everything is normal and the history fits, you're likely looking at a primary migraine. If anything feels off, don't hesitate to push for imaging or labs.
Got a story of your own? Maybe you've caught a red flag early or had a migraine that seemed "just a headache" but turned out otherwise. Share it in the comments your experience could help someone else navigate the same confusing road. And if you'd like a printable report template, grab it now and keep it in your health folder.
FAQs
What red‑flag findings should I look for during a migraine exam?
Red‑flag signs include fever, papilledema, focal neurological deficits, temporal‑artery tenderness or jaw claudication, and a sudden “thunderclap” onset.
How much time does a typical migraine physical exam take?
A quick OSCE‑style screen usually takes 5 minutes, while a more detailed neurologic exam may extend to 10–15 minutes.
When is imaging warranted for a patient with migraine‑like headaches?
Imaging (CT or MRI) is indicated if any red‑flag finding is present—such as abnormal neurologic signs, papilledema, fever, or a thunderclap onset.
What is the proper technique for assessing the temporal arteries?
Gently palpate the temporal region while the patient opens and closes the mouth; note tenderness, diminished pulse, or pain, which suggest temporal arteritis.
Is neck stiffness ever a normal finding in migraine patients?
Mild neck muscle tension can accompany migraine, but true stiffness or pain with flexion/extension suggests meningitis or another secondary cause and requires further evaluation.