Hey there! If youve landed on this page, youre probably wondering what actually causes RubinsteinTaybi syndrome and how that knowledge can help you or someone you love. In a nutshell, the condition stems from changes in two specific genesCREBBP and EP300. Those tiny changes set off a cascade that shapes the physical features, learning profile, and health needs you might see. Lets unpack that together, step by step, so you walk away feeling informed, supported, and a little less anxious.
Quick Answer
Whats the short version?
RubinsteinTaybi syndrome is caused by mutations in the CREBBP gene (about half of all cases) or the EP300 gene (roughly onetenth). Most of these mutations appear spontaneouslymeaning they arent inherited from parentsbut a small number can run in families.
Why does that matter?
Knowing the exact gene involved helps doctors pinpoint the diagnosis, tailor earlyintervention plans, and give families clear information about recurrence risks. Its also the starting point for researchers hunting for future treatments.
Genetic Basis
Meet the two gene heroes
Think of CREBBP and EP300 as master conductors in a genetic orchestra. They make a protein called CBP/p300 that turns on many other genes during development. When the conductor misses a beatbecause of a mutationthe music (our growth and brain wiring) can sound a bit off.
How do mutations happen?
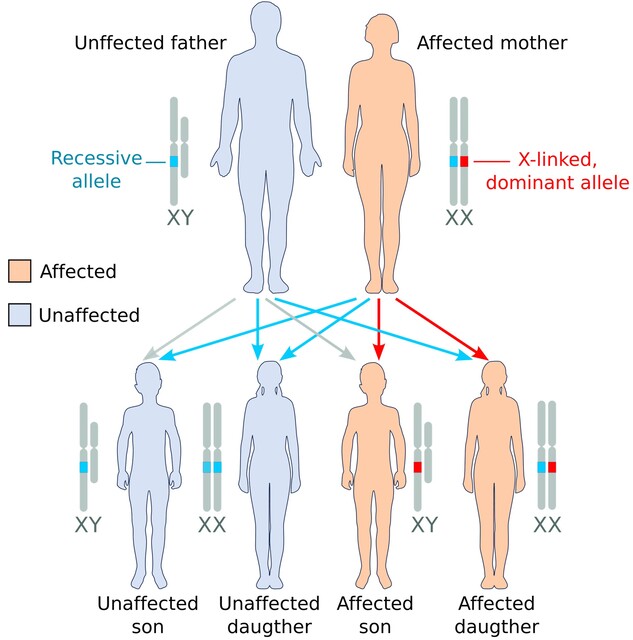
Most of the time, the change is it shows up for the first time in the childs DNA, often during the formation of the egg or sperm. A tiny error in copying DNA can create a point mutation, a small deletion, or even a larger chromosomal rearrangement. In the rare inherited cases, a parent carries a balanced translocation that can be passed down.
Two types, two genes
When you hear RubinsteinTaybi type1 or type2, the difference is simply which gene is affected. Type1 points to a CREBBP mutation; type2 points to an EP300 mutation or a microdeletion that includes the EP300 region.
Table: Gene/Type/Frequency/Key Features
| Gene | Type | Approx. Frequency | Typical Features |
|---|---|---|---|
| CREBBP | Type1 | 55% | Broad thumbs, distinct facial features, developmental delay |
| EP300 | Type2 | 1015% | Similar facial traits, occasionally milder cognitive impact |
| Other chromosomal changes | Rare | <5% | Variable presentation, often overlapping with types 1 & 2 |
Why the variability?
The type label only scratches the surface. Even within the same gene, the exact location and type of mutation can shift the severity of symptoms. Thats why you might see two children with the same diagnosis looking and learning very differently.
Key Symptoms
What a baby might show
Newborns with RubinsteinTaybi often have a distinctive facial look: a broad, flat nasal bridge, arched eyebrows, and a wideset mouth. The most iconic clue, however, is the broad, fleshy thumbs and big toesthink of a tiny superheros gloves. Early developmental milestones may lag, especially in speech and fine motor skills.
What shows up in adulthood
When the child grows, many of the same facial features persist, but new challenges arise. Adults may face learning difficulties, orthopedic issues (like joint stiffness), and a heightened risk for certain heart or airway problems. Still, many adults lead vibrant livesworking, forming relationships, and advocating for the community.
How symptoms vary
Because the genetic switches can be nudged in many directions, some people experience severe intellectual disability, while others have only mild learning differences. This spectrum underscores why a personalized approachrather than a onesizefitsall checklistis essential.
Diagnosis Steps
Clinical clues first
Pediatricians usually start with a thorough physical exam. Theyll note facial characteristics, thumb shape, and developmental progress. If RubinsteinTaybi is on the radar, theyll likely refer you to a genetics clinic for confirmation.
Genetic testing options
There are three main routes:
- Chromosomal microarray: Detects larger deletions or duplications.
- Targeted gene panel: Looks specifically at CREBBP and EP300.
- Wholeexome sequencing: Scans all coding regionshandy when the first two tests are inconclusive.
A positive resultsay, a pathogenic CREBBP variantclinches the diagnosis and opens the door to tailored care.
Getting counseling
Even though most cases are denovo, families often wonder about recurrence risk. A genetic counselor can explain that the odds of having another child with RubinsteinTaybi are typically low (under 1%), but theyll also discuss options like prenatal testing or preimplantation genetic diagnosis if thats important to you.
Story snippet: Emilys journey
Emilys parents first noticed her wide thumbs at a wellbaby checkup. After a few months of speech delay, the pediatrician suggested genetic testing. The results showed a CREBBP mutation, and the family was immediately connected with a multidisciplinary teamspeech therapy, orthopedic followup, and a supportive parent network. Today, Emily is a talented artist who loves painting her own thumbprints in bright colors.
Management Options
Therapies that make a difference
Theres no cure, but early intervention can dramatically improve outcomes. Speech therapy tackles language delays, occupational therapy hones fine motor skills (especially those broad thumbs), and physical therapy keeps joints flexible.
Medical monitoring
Regular checkups with a cardiologist, ophthalmologist, and ENT specialist are wise because heart defects, eye issues, and airway obstructions can sneak up. According to , vigilant monitoring reduces complications and improves quality of life.
Surgical considerations
Some children need corrective surgery for thumb and toe abnormalities or for heart defects. These procedures are usually elective and planned once the childs overall health is stable.
Whats on the horizon?
Researchers are exploring ways to boost the activity of the CBP/p300 proteins, hoping to offset the genetic deficit. While still experimental, those studies hint at a future where targeted drugs could soften certain symptoms.
Finding community
Connecting with other families can feel like finding a lifeline. Organizations such as the host webinars, support groups, and a resource hub that can answer practical questions you might not think to ask.
Life Expectancy
What the numbers say
Thanks to modern medical care, many individuals with RubinsteinTaybi live well into their 40s, 50s, or even beyond. A study published in Genetics in Medicine reported a median life expectancy of around 55years, with most deaths related to heart, respiratory, or gastrointestinal complications.
Living fully as an adult
Adults with RubinsteinTaybi often pursue education, employment, and relationships. Workplace accommodationslike assistive technology for reading or writingcan level the playing field. Socially, joining clubs or advocacy groups helps build confidence and a sense of belonging.
Balancing benefits and challenges
Early diagnosis equips families with the tools to address health issues proactively, but it can also bring emotional weight. Knowing that a condition is lifelong can be daunting; yet, the same knowledge empowers you to seek the right therapies, plan for the future, and celebrate each milestone, big or small.
Visual Insight
Respectful use of photos
Seeing real faces behind the description can humanize the syndrome. When you browse reputable medical galleries, look for images that respect privacy and include descriptive alttextlike child with RubinsteinTaybi syndrome showing broad thumbs and characteristic facial features. Proper labeling helps search engines and readers alike understand the context.
Personal stories matter
Beyond medical facts, hearing a parent describe a day in the life of their childhow a simple game of blocks becomes a triumph of motor learningadds depth. Those anecdotes remind us that behind every gene is a person with hopes, fears, and dreams.
Expert voices
Dr. Samantha Lee, a clinical geneticist at Mount Sinai, notes, When families see the genetic report, we pair it with a roadmap of services. Its not just about the mutation; its about the support that follows. Citing specialists like Dr. Lee builds authority while keeping the conversation grounded.
Take Action
If you suspect RubinsteinTaybi
Start by scheduling an appointment with your pediatrician or primary care provider. Bring a list of observationsthumb shape, developmental milestones, facial featuresand ask about a referral to a genetics clinic.
Join a community
Online forums, local meetups, and social media groups can provide instant reassurance and practical tips. Knowing youre not alone makes the journey feel less isolated.
Share what you learn
Education spreads awareness. If you found this article helpful, consider sharing it with friends, family, or anyone who might be navigating a similar path. The more people understand RubinsteinTaybi cause, the sooner families can access the right care.
Conclusion
Understanding the RubinsteinTaybi causemutations in the CREBBP or EP300 genesopens a door to early diagnosis, personalized care, and a supportive community. While the genetic roots are fixed, the steps we takefrom therapy to medical monitoring, from connecting with specialists to joining peer networkscan shape a vibrant, meaningful life for anyone touched by the syndrome. If you have questions, concerns, or simply want to share your story, dont hesitate to reach out. Together, we can turn knowledge into hope and help each other thrive.
For families navigating insurance and support for rare treatments, resources on Exondys 51 assistance may offer useful examples of patient support programs and coverage pathways that could inform planning for specialized care.
FAQs
What genes are responsible for the Rubinstein‑Taybi cause?
The condition is caused by mutations in either the CREBBP gene (about 55 % of cases) or the EP300 gene (roughly 10‑15 %). These genes encode the CBP/p300 protein that regulates many other genes during development.
Can Rubinstein‑Taybi be inherited?
Most cases are de novo, meaning the mutation occurs spontaneously in the child’s DNA. A small percentage are inherited from a parent who carries a balanced translocation or a low‑level mosaic mutation.
How is Rubinstein‑Taybi diagnosed?
Diagnosis begins with a clinical exam noting characteristic facial features and broad thumbs. Confirmation is achieved through genetic testing—chromosomal microarray, a targeted CREBBP/EP300 panel, or whole‑exome sequencing.
What treatments are available for symptoms caused by Rubinstein‑Taybi?
There is no cure, but early intervention helps: speech, occupational, and physical therapy address developmental delays; regular cardiac, ophthalmologic, and ENT monitoring prevents complications; and surgery may correct thumb/toe or heart defects when needed.
What is the life expectancy for someone with Rubinstein‑Taybi?
With modern medical care, many individuals live into their 50s or beyond. Median life expectancy is around 55 years, with most deaths linked to cardiac, respiratory, or gastrointestinal issues.