Short answer: Rett syndrome is almost always caused by a spontaneous (denovo) mutation in theMECP2 gene on the Xchromosome; only about1% of cases are truly inherited from a parent.Understanding this inheritance pattern helps families gauge recurrence risk, plan genetic testing, and find the right support.
Why does this matter to you? If a loved one has been diagnosed, knowing whether the mutation is new or passed down can shape decisions about future pregnancies, carrier testing, and accessing community resources. Lets dive into the details together, step by step.
Inheritance Quick Overview
What does denovo mean?
Denovo is a fancy Latin phrase that simply means new. In genetics, it describes a mutation that appears for the first time in the childs DNA, not present in either parents cells. Think of it as a typo that slipped into the script while the book was being printed the authors (parents) never wrote it, but it shows up in the final copy (the child).
How often is Rett syndrome inherited?
According to , less than1% of Rett cases are inherited. Over99% arise from a denovo mutation in theMECP2 gene.
Bottomline for families
In most families, the mutation was not passed down, so the chance of having another child with Rett is low roughly1% if the mother isnt a carrier. However, for the tiny slice of families where a parent carries the mutation, the risk jumps dramatically.
| Scenario | Inheritance Type | Approximate Frequency |
|---|---|---|
| Denovo mutation (new) | Not inherited | 99% |
| Inherited from a carrier mother | Xlinked dominant | 1% |
Rett Genetics Explained
MECP2 gene the main culprit
The MECP2 gene sits on the Xchromosome and produces a protein that acts like a master switch, turning other genes on or off during brain development. When a mutation disrupts this switch, neural communication goes offtrack, leading to the classic Rett symptoms.
Types of MECP2 mutations
Most mutations are singleletter changes (point mutations), but some are small deletions or duplications. Each variant can affect the proteins function to a different degree, which partly explains why the severity of Rett can vary so much among individuals.
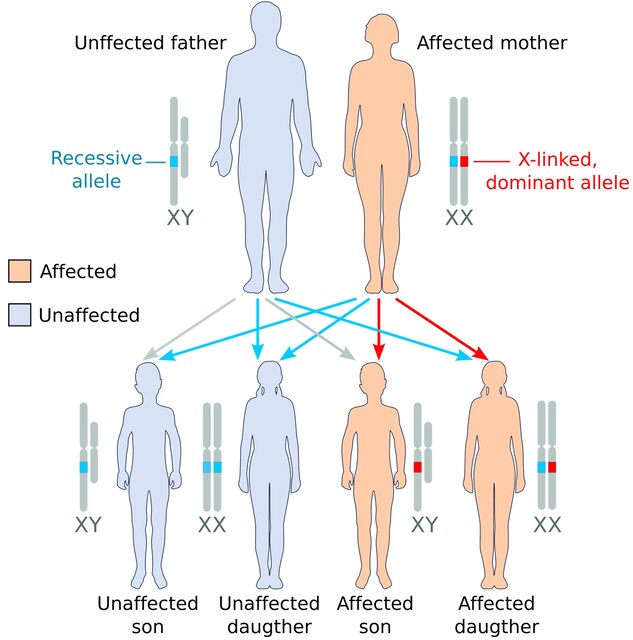
Xlinked dominant vs. recessive confusion
Rett is officially classified as an Xlinked dominant disorder. That sounds intimidating, but heres the twist: because males have only one Xchromosome, a severe MECP2 mutation is usually lethal before birth, so we rarely see affected boys. In practice, the condition appears recessive for males because the mutation doesnt survive to birth.
Dominant vs Recessive
Official classification
Rett syndrome follows an Xlinked dominant inheritance pattern. A single copy of the mutated gene on a females Xchromosome can cause the disorder, while a male with the mutation typically does not survive to term.
Why it looks recessive in practice
Because the mutation is often fatal for males, families mostly see affected girls. This makes the pattern feel recessive for boys, even though genetically its dominant. Its a subtle but important distinction when youre discussing risk with a genetic counselor.
Implications for carrier mothers and siblings
If a mother carries a pathogenic MECP2 mutation, each pregnancy carries a 50% chance of passing it to a daughter (who will develop Rett) and a 50% chance of passing it to a son (who may not survive). Siblings of an affected child have a roughly 25% chance of being carriers.
Rett Prevalence
How common is Rett syndrome?
Global estimates put Rett syndrome at about 1 in 10,00015,000 live female births. That translates to roughly 0.010.02% of the female population. The numbers can vary by region due to differences in reporting and diagnostic resources.
Regional variation
Higher prevalence rates are sometimes reported in regions with robust newborn screening programs. Conversely, underdiagnosis can occur in lowresource settings, making the true worldwide burden a bit of a mystery.
Diagnosis Process
Clinical criteria
Doctors look for a specific sequence of signs: normal early development (first 618 months), followed by a rapid loss of purposeful hand skills, spoken language, and the appearance of repetitive handwringing movements. Additional features can include seizures, breathing irregularities, and slowed growth.
Genetic testing workflow
Once clinical suspicion is high, a blood sample is sent for DNA sequencing. A targeted MECP2 panel is the fastest route, but many labs now order wholeexome sequencing, which can also catch rarer, overlapping disorders.
When to suspect a familial case
If more than one girl in a family is affected, or if a mother has subtle learning difficulties, a clinician may recommend carrier testing for the mother and possibly other female relatives. Families considering reproductive options may also discuss Rett syndrome criteria with their genetic counselor to clarify diagnostic findings.
FemaleOnly Mystery
Why does Rett mostly affect females?
The answer lies in the Xchromosome. Females have two Xchromosomes, so a mutation in one can be balanced by the normal copy, allowing them to survive but still develop the disorder. Males, with only one X, lack that backup severe mutations often result in miscarriage or stillbirth.
Rare male cases
Occasionally, boys with a milder mosaic mutation (where only some cells carry the defect) survive and display Rettlike symptoms. These cases are extremely rare but illustrate how the genetic landscape can be more nuanced than textbook definitions.
Inherited vs De Novo
Recurrence risk for future pregnancies
If genetic testing shows no parental carrier, the recurrence risk is about 1% the chance of another spontaneous mutation. If a mother is found to be a carrier, the risk climbs to 50% for each daughter and 50% for each son.
| Parental Carrier Status | Risk for Next Child |
|---|---|
| No carrier identified | 1% (new mutation) |
| Mother is a carrier | 50% for daughters (Rett), 50% for sons (often nonviable) |
When carrier testing is recommended
Guidelines from the suggest offering testing to the mother, maternal aunt, and grandmother when an inherited case is suspected. Early knowledge empowers families to explore reproductive options like preimplantation genetic diagnosis (PGD) or prenatal testing.
Preimplantation genetic diagnosis (PGD) & prenatal testing
For carrier mothers, IVF combined with PGD can screen embryos for the MECP2 mutation before transfer. During pregnancy, chorionic villus sampling (CVS) or amniocentesis can detect the mutation, providing a clearer picture early on.
Life Expectancy
Current survival statistics
Most individuals with Rett live well into adulthood; average life expectancy now exceeds 4050years, largely thanks to advances in seizure control, respiratory support, and multidisciplinary care.
Factors influencing prognosis
The specific mutation type, severity of seizures, and access to therapeutic services all play a role. Early interventionespecially speech, occupational, and physical therapycan improve quality of life and functional independence.
Success stories
There are inspiring accounts of women with Rett who have graduated from college, participated in community theater, and even advocated for research at international conferences. These stories highlight that life expectancy isnt just a number, but a narrative of possibilities.
Treatment Options
No cure, but symptombased care
Management focuses on three pillars: (1) controlling seizures with antiepileptic drugs, (2) addressing breathing irregularities (sometimes with nighttime oxygen or medications), and (3) supporting motor and communication skills through intensive therapy.
Emerging therapies
Researchers are exploring genetherapy approaches to replace the faulty MECP2 copy, as well as readthrough compounds that encourage cells to ignore premature stop signals in the gene. Earlyphase trials are ongoing, and hope is building within the community.
Support resources
Organizations like the provide families with counseling, support groups, and uptodate information on clinical trials. Connecting with these networks can make the journey feel less isolating. For practical help navigating coverage and assistance programs related to therapies, families sometimes review resources about Exondys 51 insurance to understand how specialty medication support works in similar rare-disease settings.
Conclusion
Rett syndrome is predominantly caused by a new mutation in the MECP2 gene, making true inheritance a rare exception. Understanding its Xlinked dominant nature, the tiny but real risk of passing on the mutation, and the available diagnostic and therapeutic pathways empowers families to make informed decisions. If you or someone you love is navigating Rett, remember youre not alonegenetic counselors, specialist clinicians, and supportive communities are ready to walk beside you. Feel free to share your story in the comments, download our free geneticsrisk checklist, or reach out to a certified genetic counselor for personalized guidance.
FAQs
What causes Rett syndrome?
Rett syndrome is mainly caused by a mutation in the MECP2 gene on the X chromosome, which disrupts brain development and function.
Is Rett syndrome inherited from parents?
Over 99% of Rett syndrome cases are due to new (de novo) mutations, not inherited from parents. Rarely, it can be passed from a carrier mother.
Can males get Rett syndrome?
Rett syndrome mostly affects females; males with MECP2 mutations often have severe symptoms and may not survive infancy.
What is the recurrence risk for Rett syndrome?
If no parent is a carrier, the risk is about 1%. If the mother is a carrier, each daughter has a 50% chance of being affected.
How is Rett syndrome diagnosed?
Diagnosis involves clinical evaluation and genetic testing for MECP2 mutations, especially when classic symptoms are present.