Rapidly progressive dementia (RPD) can take a loved one from the first confusing moment to the end of life in just monthsor, in some cases, only weeks. The speed of decline is shocking, and many families wonder how quickly it can become fatal.
While a handful of causes are treatable if caught early, most forms have no cure. Early recognition, a thorough workup, and compassionate end-of-life planning are the only ways to keep the person as comfortableand as dignifiedas possible.
What Is Rapidly Progressive Dementia?
Definition and how it differs from typical dementia
Typical Alzheimer's or vascular dementia usually unfolds over several years. In contrast, RPD is defined by a noticeable decline in cognition, behavior, or function that occurs within 12 months of symptom onset. The change is brisk, often catching families off guard.
Typical timeline: weeks, months, or a few years
Most patients experience a rapid plunge within 36 months, followed by a plateau that can last anywhere from a few weeks to a year before death. The exact speed depends heavily on the underlying causesome are fatal within weeks (like CreutzfeldtJakob disease), while others (certain autoimmune encephalitides) may linger longer if treated.
Why rapidly progressive dementia death matters
Understanding that RPD can lead to death much faster than regular dementia helps families seek urgent medical attention, set realistic expectations, and make informed decisions about care and legal matters.
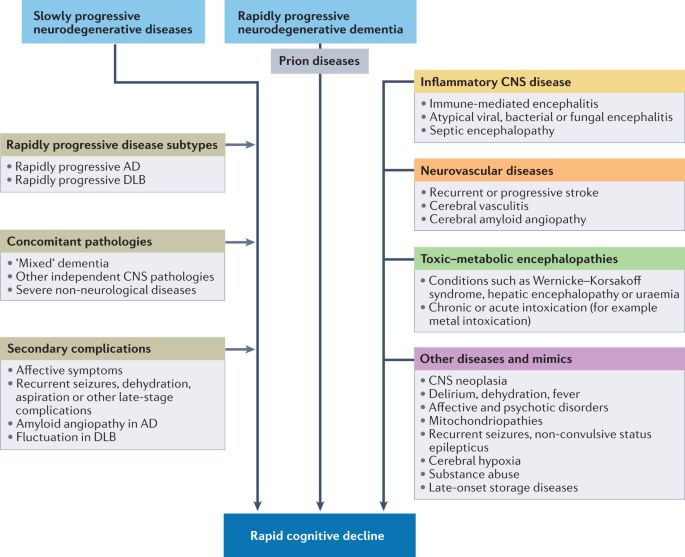
Main Causes Explained
Neurodegenerative diseases
Prion disorders such as CreutzfeldtJakob disease (CJD) are the classic culprits. Atypical presentations of Alzheimer's or Lewy-body disease can also progress rapidly.
Autoimmune and inflammatory conditions
Hashimoto's encephalopathy, anti-NMDA receptor encephalitis, and vasculitis can mimic RPD. When diagnosed early, immunotherapy (steroids, IVIG) can halt or even reverse decline.
Infections and metabolic disturbances
Viral encephalitis (HSV-1), severe vitamin B12 deficiency, or Wernicke's encephalopathy can cause a sudden cognitive collapse. Prompt antimicrobial or nutritional treatment often yields dramatic improvement.
Toxic and medication-related triggers
Heavy metals, certain chemotherapy agents, or anticholinergic drug overload can precipitate rapid dementia-like symptoms. Removing the offending agent is the first step.
Comparison of reversible vs. non-reversible causes
| Cause | Typically Reversible? | Typical Survival Without Treatment |
|---|---|---|
| CreutzfeldtJakob disease | No | 412 months |
| Autoimmune encephalitis | Yes (often) | Variablemonths to years with therapy |
| HSV encephalitis | Yes (with antivirals) | Weeks to months if untreated |
| Severe B12 deficiency | Yes (with supplementation) | Months; often stabilizes |
Seeing a pattern? If the cause is treatable, the story can change dramatically. That's why a meticulous diagnostic workup is essential.
Red-Flag Signs
Sudden memory loss in less than six months
When someone you love forgets their own address, beloved pet's name, or how to button a shirt within a few weeks, it's a clear alert.
Rapid language breakdown and visual hallucinations
Often the first clue is a once-fluent speaker suddenly babbling or seeing things that aren't there. These are classic signs of rapid onset dementia.
Loss of basic self-care
Needing assistance with dressing, eating, or using the bathroom when they previously managed independently signals that the disease is accelerating.
Behavioural spikes: agitation, aggression, or apathy
These mood swings can be frightening, but they're part of the brain's frantic attempt to cope with rapid injury.
Quick checklist for caregivers
- Memory lapses that get worse each week
- Speech that becomes garbled or absent
- Hallucinations or delusions
- Inability to perform daily tasks
- Sudden mood changes
If three or more appear within a short span, consider rushing to a neurologisttime truly is brain.
Timeline to Death
Median survival by etiology
Studies show that for noncurable prion diseases, median survival hovers around 812 months. Autoimmune causes, when treated promptly, can extend life expectancy to several years. Metabolic or infectious origins usually improve with therapy, pushing the timeline beyond the initial rapid phase.
Factors that shorten survival
Advanced age, involvement of the thalamus (a deep brain hub), and severe comorbidities such as heart failure or uncontrolled diabetes can accelerate the decline. A quick glance at a recent case series shows that patients over 80 with thalamic lesions often die within six months.
Visualising the range
Imagine a bar chart where CJD peaks at 412 months, autoimmune encephalitis spreads from 6 months to 3 years, and treatable infections can stretch beyond a year if the right drugs are given.
Diagnostic Workup Steps
First-line labs and imaging
Blood work (CBC, metabolic panel, thyroid, vitamin B12) rules out reversible metabolic issues. An MRI is the golden imaging toollooking for diffusion restrictions, basal ganglia changes, or inflammatory patterns.
Advanced testing for a definitive answer
When the MRI is ambiguous, a lumbar puncture can reveal CSF markers: 14-3-3 protein or RT-QuIC positivity suggests prion disease; oligoclonal bands point toward autoimmune inflammation. PET scans sometimes highlight frontotemporal hypometabolism that MRI misses.
Decision-tree flowchart (simplified)
- Start: Sudden cognitive decline Order basic labs + MRI.
- If MRI normal but suspicion high CSF analysis.
- If CSF suggests infection Start antivirals/antibiotics.
- If autoimmune markers present Begin immunotherapy.
- If prion markers positive Discuss prognosis and palliative care.
Treatment And Care Options
Disease-specific therapies
Autoimmune encephalitis often responds to high-dose steroids, plasma exchange, or rituximab. HSV encephalitis is a clear case for IV acyclovir. Unfortunately, prion diseases lack disease-modifying drugs, so the focus shifts to comfort.
Palliative symptom management
Agitation can be eased with low-dose atypical antipsychotics, while dysphagia may require speech therapy guidance or a feeding tube. Pain, constipation, and sleep disturbances each need gentle, tailored treatment.
Clinical trials and research networks
Many academic centers run RPD registries that match patients with experimental protocols. If you're in a major city, ask your neurologist about enrolmentit's often the only way to access cutting-edge interventions.
Life Expectancy & Planning
Typical expectancy by cause
- CreutzfeldtJakob disease: 412 months
- Autoimmune encephalitis (treated): months to years
- Severe metabolic deficiency (treated): variable, often >1 year
- Typical rapid-onset Alzheimer's variant: 1224 months
Advance directives, POLST, and hospice
Getting legal documents in place early spares families later frantic phone calls. A POLST (Physician Orders for Life-Sustaining Treatment) form lets you specify whether you want CPR, intubation, or only comfort measures. Hospice can begin when life expectancy falls under six months, and it offers a team of nurses, chaplains, and social workers who specialize in the end-of-life phase.
Supporting caregivers
Watching a loved one deteriorate rapidly is emotionally exhausting. Support groupsboth in-person and onlineprovide a space to vent, learn, and feel less alone. Organizations like the Alzheimer's Association and the UCSF Memory Center have dedicated helplines for crisis moments.
Useful Resources Guide
Authoritative sites for deeper dives
UCSF's Memory and Aging Center offers clear explanations of RPD causes and workup strategies. The National Institute on Aging provides up-to-date guidelines on dementia care, while specific lab pages detail CSF tests you might encounter.
Recent peer-reviewed studies
For the science-curious, key articles include a 2022 review in BMC Geriatrics on survival trends, a 2021 Nature paper on autoimmune encephalitis biomarkers, and a 2020 Continuum article discussing palliative pathways for prion disease.
Helplines and community links
- Alzheimer's Association 24/7 Helpline: 1-800-272-3900
- UCSF Memory and Aging Center: (415) 555-1234
- National Institute on Aging:
Conclusion
Rapidly progressive dementia death is a harsh reality that can arrive far quicker than most families expect. By recognizing the red-flag signs, understanding the spectrum of causes, and pursuing an urgent, thorough workup, you gain the best chance to uncover any treatable condition and to plan for a dignified end-of-life journey.
If you suspect a rapid decline in someone you love, reach out to a neurologist todaytime truly matters. Share this guide with anyone facing a similar challenge, and feel free to ask questions or share your own story. Together, we can navigate this unsettling terrain with compassion, knowledge, and hope.
For families navigating insurance or assistance for rare or high-cost neurologic treatments, resources on Exondys 51 assistance may offer helpful models for locating patient support programs and navigating coverage discussions.