In the next few minutes Ill walk you through why ceftriaxone tops the list, what the alternatives are, and how guidelines shape the decision. Well keep it friendly, practical, and packed with the details you needno jargon overload, just clear, compassionate information.
What Makes Best Antibiotic
Efficacy Against Common Pathogens
Most bacterial meningitis cases in adults and kids are caused by Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae. Ceftriaxone hits all three with high kill rates, which is why its the goto in emergency rooms worldwide.
CSF Penetration
Antibiotics have to cross the bloodbrain barrier to reach the cerebrospinal fluid (CSF). Ceftriaxones chemical structure lets it flood the CSF at therapeutic levels, even when the meninges are inflameda crucial factor that many oral antibiotics for meningitis simply cant match.
Safety & Tolerability
Sideeffects exist for any drug, but ceftriaxone is generally welltolerated. Its given once or twice daily, which is a relief compared to more frequent dosing schedules. Allergic reactions are rare, and the drug doesnt usually require routine bloodlevel monitoring.
Guideline Endorsement
Major health bodiesCDC, WHO, and the UK NICE list ceftriaxone as firstline therapy in their guidance. When the experts line up, you can feel confident youre on the right track.
| Criteria | Ceftriaxone | Cefotaxime | PenicillinG | Vancomycin |
|---|---|---|---|---|
| Pathogen Coverage | Broad (S.pneumoniae, N.meningitidis, H.influenzae) | Similar to ceftriaxone | Limited, needs susceptibility | Grampositive + MRSA coverage |
| CSF Penetration | Excellent | Excellent | Good if meninges inflamed | Variable |
| Dosing Frequency | Once/ twice daily | Four times daily | Every 46h | Every 612h (levelguided) |
| Common Sideeffects | Biliary sludging, rash | Similar to ceftriaxone | Allergic reactions | Nephrotoxicity, ototoxicity |
FirstLine Choice Ceftriaxone
Dosage & Duration
For adults, the standard is 2g IV or IM every 12hours, usually continued for 1428days depending on the organism and clinical response. Kids get a weightbased doseroughly 100mg/kg per day, split into two doses.
Evidence Snapshot
According to a recent review, ceftriaxone achieved cure rates above 90% for communityacquired meningitis, outperforming older penicillin regimens. The same study highlighted its superior CSF concentrations, reinforcing why its the champion.
Benefits
- Broadspectrum coverage against the usual suspects.
- Oncedaily dosing is possible for some patients, which eases nursing workload.
- Welldocumented safety profile.
Risks & Contraindications
Watch out for biliary sludgeespecially with prolonged therapy. Allergic reactions, though rare, can be severe. Also, dont mix ceftriaxone with calciumcontaining solutions (think certain pediatric IV fluids) because it can precipitate in the bloodstream.
Common Alternatives Explained
When Ceftriaxone Isnt an Option
Allergies happen. Some patients have betalactam hypersensitivity, while others live in regions with high resistance to thirdgeneration cephalosporins. In those cases, clinicians turn to alternatives that still meet the four criteria we discussed earlier.
Oral Antibiotics for Meningitis
Oral therapy is rare, but after a solid IV course and once the pathogen proves susceptible, drugs like doxycycline can be used for stepdown. Its convenient, but you must finish the full IV phase firstno shortcuts.
Pediatric Nuances
Neonates (under 2months) get cefotaxime instead of ceftriaxone because the latter can displace calcium and cause jaundice. Dosing is weightbased, and most guidelines recommend adding ampicillin to cover Listeria when needed.
AdultSpecific Nuances
In adults, rising penicillinresistant S.pneumoniae means vancomycin is often added to ceftriaxone until susceptibility results return. This combo guards against resistant strains without delaying treatment.
QuickReference Cheat Sheet
Below is a concise look at when you might choose each drug.
| Antibiotic | Typical Use | Key Advantage | Main Caveat |
|---|---|---|---|
| Ceftriaxone | Firstline, all ages | Broad, oncedaily possible | Allergy, biliary sludge |
| Cefotaxime | Neonates, infants | Safe for newborns | More frequent dosing |
| PenicillinG | Susceptible S.pneumoniae | Cheap, long history | Needs susceptibility data |
| Vancomycin | Resistant Grampositives | Covers MRSAlike strains | Nephrotoxicity, monitoring |
| Doxycycline | Oral stepdown | Good CSF penetration | Not for pregnancy, photosensitivity |
Guidelines Shape Choice
US (IDSA/CDC) Guidelines
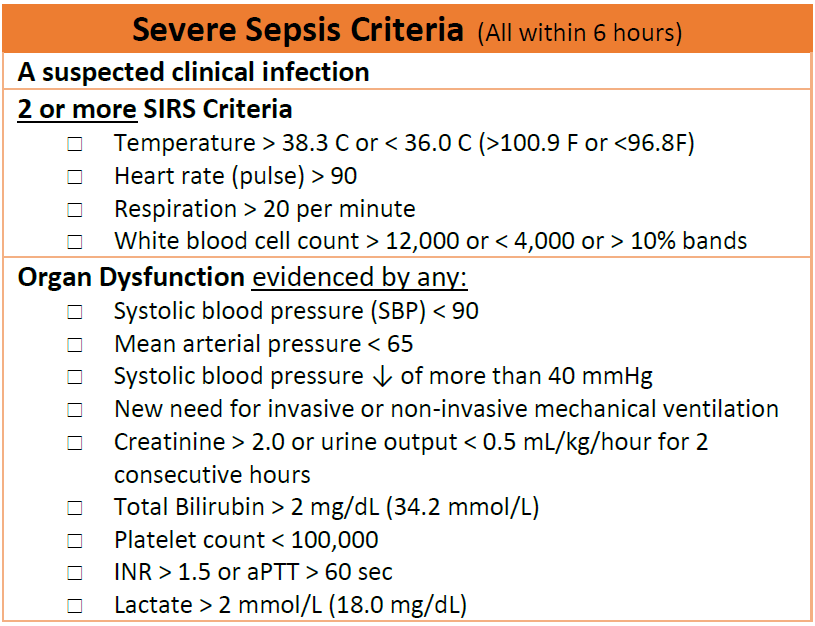
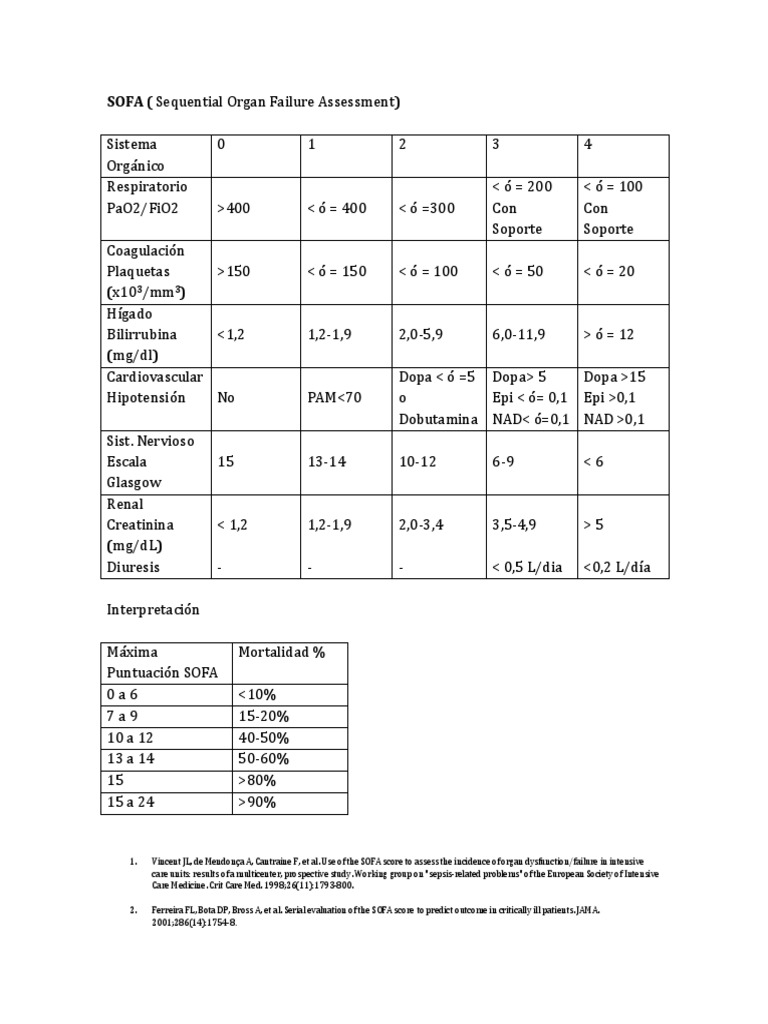
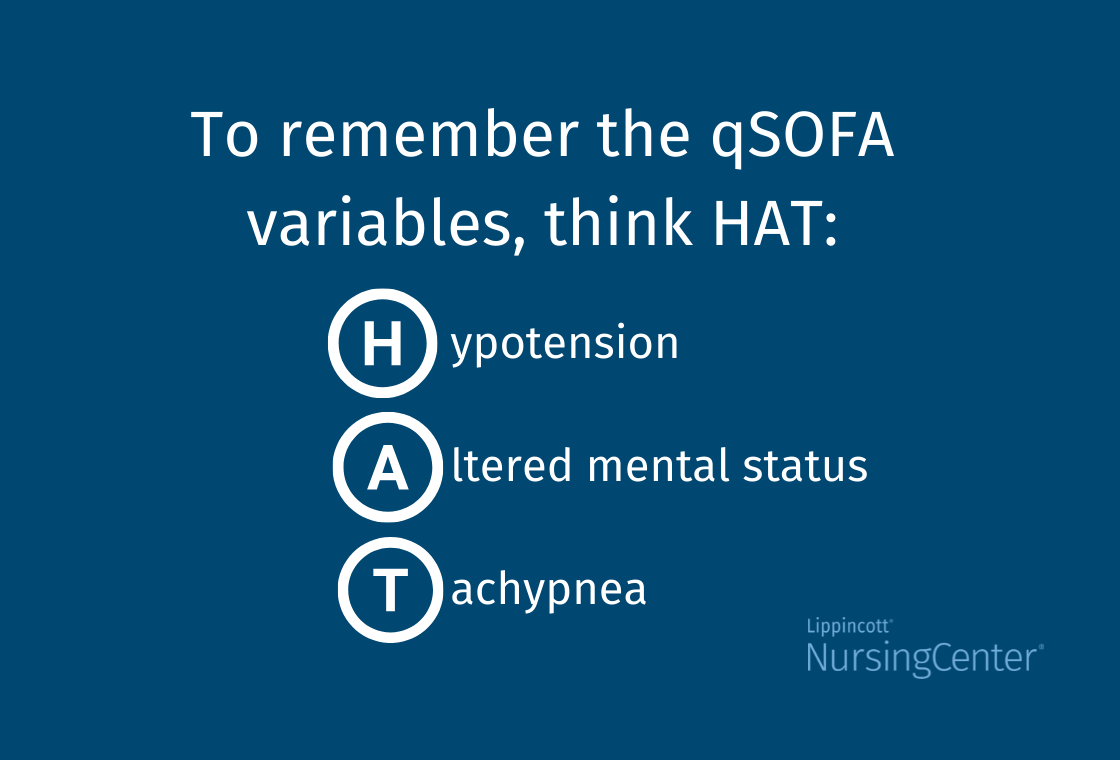
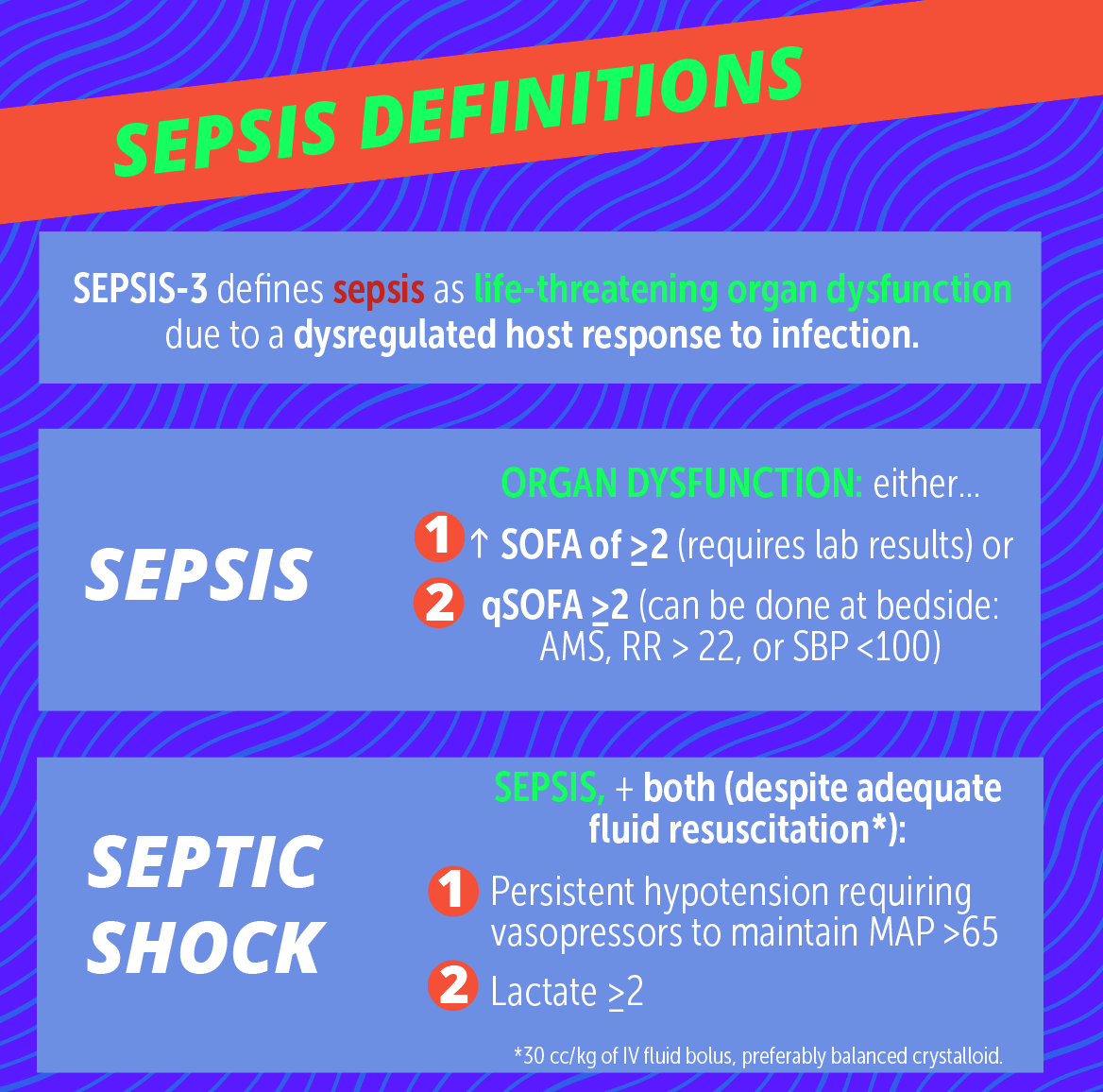
The Infectious Diseases Society of America (IDSA) and CDC both list ceftriaxonevancomycin as the empiric regimen for adults. Their guidance emphasizes rapid initiationtime is brain. For clinicians wanting a concise overview of sepsis severity and organ dysfunction that often accompanies meningitis, tools like the sepsis severity assessments can be helpful adjuncts when evaluating a critically ill patient.
European & UK Guidance
EUCAST and NICE mirror the US stance, adding dexamethasone for pneumococcal meningitis to reduce neurological sequelae. The NICE document (available as a PDF on their website) provides clear dosing charts for both children and adults.
WHO & LowResource Settings
In many developing countries, ceftriaxone may be scarce, so chloramphenicol or highdose doxycycline are recommended. The WHOs Essential Medicines List still highlights ceftriaxone as the preferred agent when available.
Where to Find Full PDFs
If you love digging into the original documents, the CDC and NICE sites both host downloadable PDFs. Just search meningitis treatment guidelines pdf on their portals for the most recent version.
Decision Tree Benefits Risks
StepbyStep Flow
- Suspect meningitis Get CSF sample ASAP.
- Start empiric therapy Ceftriaxone+vancomycin (adults) or cefotaxime+ampicillin (neonates).
- Review culture results Deescalate to the narrowest effective drug.
- Assess response If stable after 4872h, consider oral stepdown if pathogen is susceptible.
- Complete full course Usually 1428days, adjusted for organism and complications.
When to Switch to Oral
A switch is safe only when the patient is afebrile, neurologically stable, and the isolate is known to be sensitive to an oral agent like doxycycline. This transition shortens hospital stay and eases the burden on families.
Monitoring & FollowUp
Watch renal function if vancomycin is used, liver enzymes for ceftriaxone, and hearing tests for any ototoxic drug. Early detection of sideeffects can prevent longterm damage.
RealWorld Experience Stories
Adult Case: Quick Recovery
John, a 34yearold marathon runner, arrived with fever, headache, and a stiff neck. Within an hour the ER started ceftriaxone. Cultures later grewN.meningitidis, confirming the choice. Johns fever broke in 18hours, and he walked out after a 10day IV courseno lingering deficits.
Pediatric Case: Infant Nuance
Little Mia, 6months old, presented with vomiting and bulging fontanelle. Because she was under 2months, the team gave cefotaxime plus ampicillin. The pathogen wasE.coli, resistant to ceftriaxone but sensitive to cefotaxime. Mia recovered fully after a 21day regimen.
Allergy Scenario: Creative Solution
Mark, 52, has a documented severe reaction to all betalactams. The team used meropenem combined with highdose doxycycline. After 14days, his CSF cleared, and he was switched to an oral doxycycline taper. Marks story shows that even without the best drug, effective alternatives exist.
Sources & Further Reading
All the information above pulls from reputable, uptodate sources:
- CDC Clinical Guidance for Meningitis (official).
- UK NICE Guidelines on Bacterial Meningitis.
- WHO Essential Medicines List (latest edition).
- Peerreviewed article Management of Acute Meningitis (PMCID9594998).
- Clinical reviews from Mayo Clinic Proceedings and Medscape.
Conclusion
When you put the pieces togetherbroad coverage, solid CSF penetration, safety, and strong guideline backingceftriaxone unmistakably shines as the best antibiotic for meningitis. Yet the story doesnt end there. Real patients have allergies, special agerelated needs, and local resistance patterns that demand a flexible, evidencebased approach.
Understanding the benefits, risks, and alternatives equips you (or a loved one) to have an informed conversation with your healthcare team. If youve faced meningitisor are supporting someone who haswhat did your experience teach you about treatment choices? Share your thoughts below, ask questions, or drop a note about what helped you feel confident during such a scary time.
Remember, knowledge is a powerful ally. Stay curious, stay safe, and dont hesitate to reach out to a medical professional for personalized advice.
FAQs
What makes ceftriaxone the best antibiotic for meningitis?
Ceftriaxone offers excellent CSF penetration, broad coverage against the most common meningitis pathogens, and a convenient dosing schedule with a well‑documented safety profile.
How quickly should treatment be started when meningitis is suspected?
Antibiotic therapy should begin within the first hour of suspicion because every minute of delay can increase the risk of neurological damage.
Are there situations where ceftriaxone cannot be used?
Yes—patients with severe beta‑lactam allergies, documented resistance, or in neonatal cases (where cefotaxime is preferred) may need alternative agents.
When is it appropriate to switch from IV to oral antibiotics for meningitis?
Switch to oral therapy only after the patient is afebrile, neurologically stable, and the causative organism is proven susceptible to an oral agent such as doxycycline.
What additional drug is often added to ceftriaxone for adult meningitis?
Vancomycin is commonly added empirically to cover penicillin‑resistant Streptococcus pneumoniae and other resistant Gram‑positive organisms until culture results are available.