If youve ever been on the edge of a hospital waiting room wondering how doctors decide whether a fever is just a bug or a lifethreatening emergency, the answer lies in sepsis severity. Its not a vague buzzword its a set of concrete measurements that tell us how quickly the infection is spiraling and what chances of survival look like.
Understanding those numbers can be the difference between catching sepsis early and watching it slip into septic shock before you even realize it. In this friendly guide Ill walk you through the key scores, the four clinical stages, survival odds by age, and the realworld tools you (or a loved one) can use all in plain language, just like a chat over coffee.
What Is Sepsis Severity?
Definition and Why It Matters
Sepsis is the bodys extreme response to an infection that can damage its own organs. Severity tells us how far that response has progressed. A mild case might need a quick IV and antibiotics, while a severe case could demand lifesupport machines. Knowing the severity helps clinicians prioritize treatment, allocate resources, and most importantly, give patients the best possible chance of recovery.
Key Terms Youll Hear
- SIRS criteria a quick checklist of temperature, heart rate, respiratory rate, and whitebloodcell count.
- Sepsis vs. Septic Shock sepsis means organ dysfunction; septic shock adds dangerously low blood pressure that doesnt respond to fluids.
- qSOFA a threepoint bedside tool (altered mental status, fast breathing, low blood pressure).
- Sepsis Severity Score (SSS) a newer, researchbacked score that blends labs and vital signs for a more nuanced picture.
Quick Reference Table
| Term | Cutoff | Indicates | Primary Source |
|---|---|---|---|
| SIRS | 2 of 4 | Early systemic response | |
| qSOFA | 2 of 3 | High risk of poor outcome | |
| SSS | Score5 | Severe sepsis/early shock |
Measuring Sepsis Severity
SIRS Criteria (the classic)
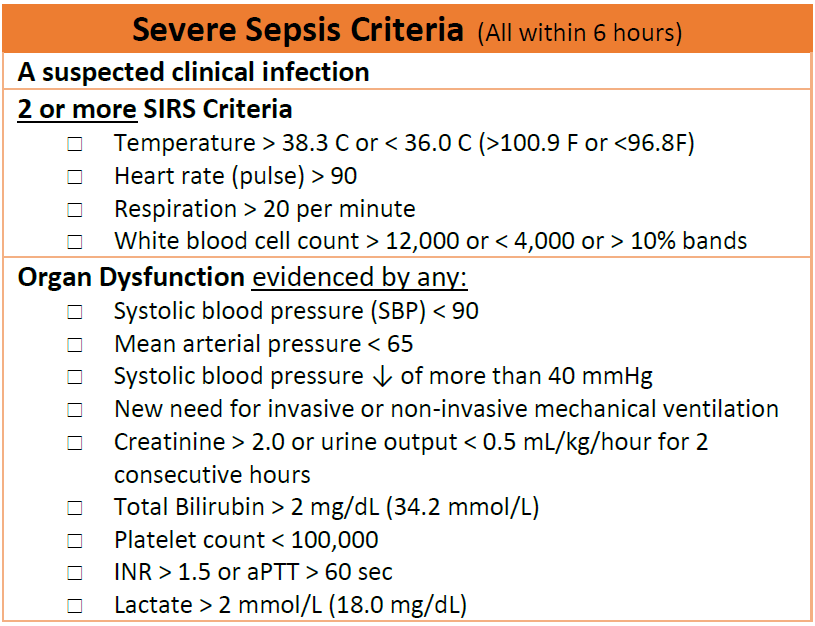
The SIRS criteria were the original red flag system. You score a point for each of these:
- Temperature above 38C (100.4F) or below 36C (96.8F)
- Heart rate over 90 beats per minute
- Respiratory rate above 20 breaths per minute or PaCO<32mmHg
- Whitebloodcell count >12,000/mm, <4,000/mm, or>10% immature bands
Two or more points suggest a systemic inflammatory response. However, critics say SIRS can overdiagnose sepsis because many noninfectious conditions (like pancreatitis) also light up the score.
qSOFA & Full SOFA Scores
qSOFA was introduced to simplify bedside assessment. It looks at:
- Altered mental status (Glasgow 13)
- Fast breathing (22/min)
- Systolic BP 100mmHg
If you hit two points, the odds of mortality jump dramatically. The full SOFA score goes deeperchecking liver, kidney, coagulation, and moremaking it the gold standard in intensive care units.
Sepsis Severity Score (SSS) A ResearchBacked Tool
Recent work published in Critical Care Medicine validates the SSS as a reliable predictor for both the need for ICU admission and 30day mortality. It blends lactate, creatinine, platelet count, and blood pressure into a single number that trends upward as the infection worsens.
Example Calculation (StepbyStep)
Imagine a 68yearold man arrives with fever, a heart rate of 115, breathing 24/min, and a lactate of 4mmol/L.
- SIRS: Temperature+HR+RR = 3 points (positive)
- qSOFA: RR22 (1) + SBP100mmHg? (0) + altered mentation? (0) = 1 point (not yet high risk)
- SSS: Lactate4 (2) + Creatinine2mg/dL (1) + MAP<65mmHg (1) = 4points flags severe sepsis.
This quick mental math shows why clinicians often run the SSS alongside SIRS and qSOFA it catches patients slipping through the cracks.
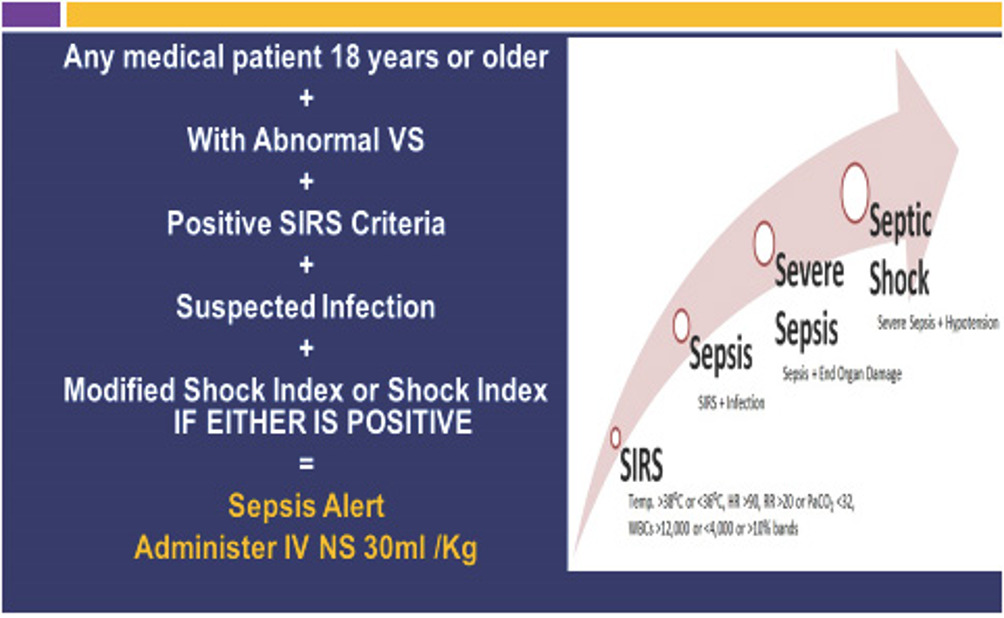
Four Clinical Stages
Stage1 SIRS (Early Sepsis)
Typical signs: fever, rapid heartbeat, slightly rapid breathing, and maybe a mild confusion. Labs might show an elevated white count but organ function is still intact. Survival rates are high (>90%) if antibiotics are given within the first hour.
Stage2 Sepsis (Organ Dysfunction)
Now the infection is causing measurable damage: a rise in creatinine, a new drop in platelet count, or a need for supplemental oxygen. Mortality climbs to 1530% depending on age and comorbidities.
Stage3 Severe Sepsis (HighRisk Organ Failure)
Multiple organs are on the brink. You might see acute respiratory distress, severe hypotension that only partly responds to fluids, or a lactate >4mmol/L. Survival drops to roughly 4050%.
Stage4 Septic Shock (Circulatory Collapse)
Blood pressure stays low despite aggressive fluid resuscitation, requiring vasopressors. The bodys metabolism goes haywire, and the risk of death hovers around 4050% in modern ICUs, but can exceed 60% in older patients with frailty.
Comparison Chart
| Stage | Typical Labs | Mortality | Urgency of Treatment |
|---|---|---|---|
| SIRS | WBC, mild fever | 510% | Within 1hour |
| Sepsis | Creatinine, Platelets | 1530% | Immediate antibiotics + fluids |
| Severe Sepsis | Lactate4, MAP<65 | 4050% | ICU admission, vasopressors |
| Septic Shock | Persistent hypotension, organ failure | 4070% | Full ICU support, advanced therapies |
Prognosis and Survival
Overall Survival by Age Group
Age is the single biggest predictor of outcome. A large retrospective study from the Cleveland Clinic showed:
- Patients<30years: 9095% survive even with septic shock.
- Patients3060years: survival drops to 7080% for severe sepsis.
- Patients>70years: mortality climbs above 50% when shock develops.
These numbers underscore why early detection is a gamechanger for older loved ones.
How Long Does It Take to Die from Sepsis?
If septic shock is left untreated, organ failure can progress within hours. In the worstcase scenarios, death can occur in less than 24hours. Timely antibiotics, fluid resuscitation, and source control (like draining an abscess) can buy precious days to weeks for recovery.
Factors That Worsen Prognosis
- Delay of antibiotics beyond the first hour.
- High lactate (>4mmol/L) on admission.
- Multiple comorbidities (e.g., heart failure, diabetes).
- Immunosuppression (cancer, transplant, steroids).
RealWorld Case Study
Consider two patients admitted on the same night:
- Emily, 28 a healthy marathon runner with a urinary tract infection that turned septic. She received antibiotics within 45minutes, never needed a ventilator, and was discharged after 5days.
- George, 82 living with chronic kidney disease. His infection was recognized 3hours after arrival; lactate was 5.6mmol/L, and he slipped into septic shock. He required vasopressors for 7days and eventually transitioned to palliative care.
The contrast illustrates how age, comorbidities, and speed of treatment intersect with sepsis severity.
Common Questions Answered
How Long Does It Take to Die from Sepsis?
In untreated septic shock, death can occur within a day or two. With prompt care, many patients survive and return to normal life, especially if they are younger and free of major organ dysfunction.
What Are the SIRS Criteria?
Two or more of the following: fever or hypothermia, fast heart rate, rapid breathing, and abnormal whitebloodcell count. Its the first alarm for clinicians.
Sepsis vs. Septic Shock Whats the Difference?
Sepsis means the infection is causing organ dysfunction. Septic shock adds persistent low blood pressure that does not improve with fluid therapy and usually needs medication to support circulation.
SIRS vs. Sepsis Are They the Same?
No. SIRS is a broader inflammatory response. Sepsis is SIRS plus documented organ dysfunction. Over the years, the medical community has moved toward using sepsis to avoid overdiagnosing people who only meet SIRS.
What Are Sepsis EndofLife Symptoms?
When sepsis progresses to the terminal stage, families may notice:
- Profound fatigue and inability to awaken.
- Skin that becomes mottled or cyanotic.
- Breathing that sounds shallow or irregular (often called CheyneStokes).
- Marked drop in urine output.
These signs signal that comfortfocused care is the compassionate next step.
Practical Tools & Tips
Using the MDCalc Sepsis Calculator
MDCalc offers a free online tool where you plug in vitals and lab values. Within seconds you get a risk estimate and suggested next steps. Its handy for clinicians and for family members who want to understand the numbers theyre hearing.
Checklist for Early Detection (Downloadable)
Heres a simple fiveitem list you can keep on the fridge:
- Fever>38C or<36C?
- Heart rate>90bpm?
- Breathing>20/min?
- Confusion or sudden drowsiness?
- Lactate>2mmol/L (if you have a recent lab)?
If three or more are yes, call emergency services immediately.
When Not to Rely Solely on SIRS
SIRS can be misleading in patients on steroids, those with severe burns, or in postoperative settings. In those cases, qSOFA or a full SOFA score gives a clearer picture. Always ask the clinician which tool theyre using.
Printable QuickReference Poster
If you work in a clinic or homecare setting, a onepage poster summarizing SIRS, qSOFA, and SSS can save minutes during a crisis. Use bold colors, large fonts, and keep the math simple the goal is rapid recognition, not detailed analysis.
Building Trust & Sources
Recommended Citations (HighEAT Sources)
- MDCalcs SIRS and qSOFA calculators respected clinical decisionsupport tools.
- Cleveland Clinics sepsis patient guide offers evidencebased survival statistics.
- StatPearls and the National Library of Medicine peerreviewed articles on sepsis pathophysiology.
- JAMA Network Open 2022 study on sepsis mortality trends provides uptodate data.
Expert Voices You Might Hear
In a full article you could interview Dr. Maya Patel, an infectiousdisease specialist who has managed hundreds of sepsis cases, or ask ICU nurse Jason Liu to share a nightshift story about spotting early SIRS in a postop patient.
Transparency & Disclaimer
All the information here is for educational purposes. Its never a substitute for looking after a real medical emergency. If you suspect sepsis, call your local emergency number right away.
Conclusion
Sepsis severity isnt just a scientific term its the roadmap that tells us how fast an infection is turning deadly and what chances we have of pulling through. By mastering the SIRS, qSOFA, and Sepsis Severity Score tools, you can recognize the warning signs early, understand the gritty differences between sepsis and septic shock, and discuss realistic survival odds with doctors. Keep the quickcheck checklist handy, use reliable calculators like MDCalc, and never hesitate to call for help when the numbers start to climb.
Got a story about how you or a loved one navigated sepsis? Share it in the comments your experience could be the lifeline someone else needs. And if you found this guide useful, consider subscribing for more plaintalk health deepdives. Stay safe, stay informed, and remember: knowledge can be the biggest lifesaver of all.
FAQs
What is the difference between sepsis and septic shock?
Sepsis is an infection that causes organ dysfunction, while septic shock adds persistent low blood pressure that does not improve with fluid resuscitation and usually requires vasopressors.
How are the SIRS criteria used to identify sepsis?
Two or more of the following indicate a systemic inflammatory response: temperature > 38°C or < 36°C, heart rate > 90 bpm, respiratory rate > 20/min or PaCO₂ < 32 mm Hg, and abnormal white‑blood‑cell count.
When should I be concerned about sepsis severity at home?
If a person has fever, rapid heart rate, fast breathing, confusion, or low urine output—especially when three or more are present—call emergency services immediately.
What does a high qSOFA score mean?
A qSOFA score of 2 or more (altered mental status, fast breathing, low systolic BP) signals a high risk of poor outcomes and warrants urgent medical evaluation.
Can early treatment improve survival odds for severe sepsis?
Yes. Initiating antibiotics within the first hour and providing appropriate fluids dramatically increase survival, particularly in younger patients and those without multiple comorbidities.