Short answer: SIRS (Systemic Inflammatory Response Syndrome) is the bodys alarm system that can be set off by anything from a broken bone to a feverish infection. When that alarm rings and an infection is present, it becomes sepsis, and if the infection overwhelms the circulatory system it can progress to septic shock.
Hey there! Im Dr. AnaMartnez, an emergencyroom physician whos spent more than a decade watching these alarms go off, sometimes harmlessly and sometimes turning into lifethreatening emergencies. Lets sit down, grab a coffee, and sort out the confusion aroundsirs vs sepsis together.
What Is SIRS
What does SIRS stand for and why does it matter?
SIRS = Systemic Inflammatory Response Syndrome. Its the bodys red flag that something is wrong, whether its an infection, a major injury, or even pancreatitis. Recognizing it early helps clinicians hunt down the cause before things get messy.
What are the official SIRS criteria?
According to the classic 1992 consensus (see ), a patient meets SIRS if two or more of the following are present:
| Criterion | Threshold |
|---|---|
| Body temperature | >38C (100.4F) or <36C (96.8F) |
| Heart rate | >90 beats per minute |
| Respiratory rate | >20 breaths per minute OR PaCO <32mmHg |
| Whitebloodcell count | >12,000cells/L, <4,000cells/L, or >10% immature (band) forms |
How is SIRS diagnosed in practice?
In the emergency department we usually start with vital signs and a quick CBC. If at least two criteria are met, the patient is flagged as SIRS and we begin looking for the underlying triggerinjury, burn, pancreatitis, or infection.
Can SIRS occur without infection?
Absolutely. Trauma, major surgery, burns, and even severe allergic reactions can light up the SIRS alarm. Thats why the infection piece is the key differentiator when we move toward sepsis.
What Is Sepsis
How does the new Sepsis3 definition differ?
In 2016 the Sepsis3 consensus redefined sepsis as lifethreatening organ dysfunction caused by a dysregulated host response to infection. Instead of relying on SIRS alone, clinicians now use the SOFA score (Sequential Organ Failure Assessment)an increase of 2 points signals sepsis. For quick bedside screening, the qSOFA (quick SOFA) looks at mental status, systolic BP 100mmHg, and respiratory rate 22.
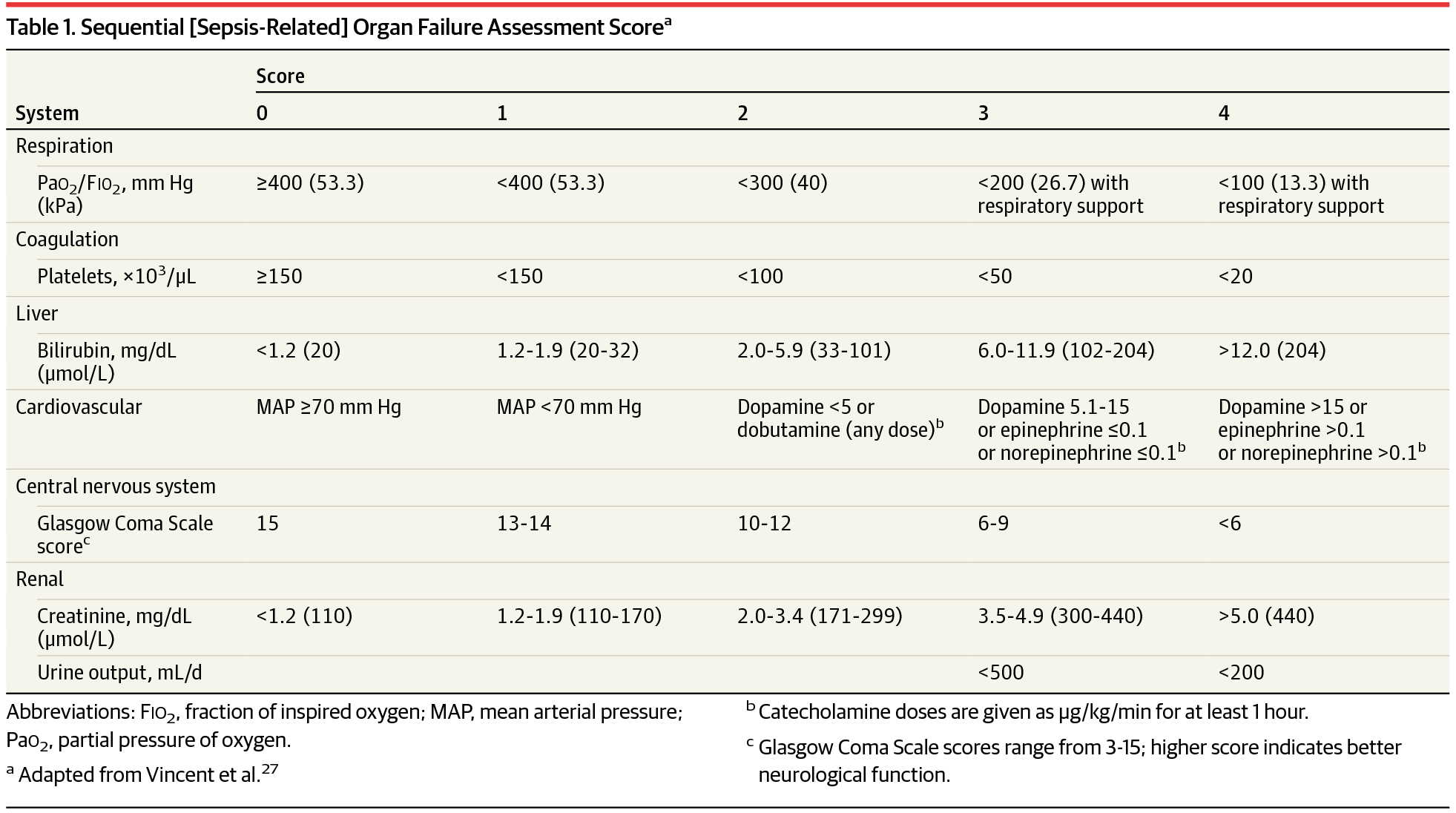
What are the Sepsis criteria (organdysfunction scores)?
The full SOFA score evaluates six organ systems (respiratory, coagulation, liver, cardiovascular, CNS, renal). Each organ gets 04 points; a rise of two or more points from baseline suggests sepsis. Heres a snapshot from the :
| Organ System | Score 0 | Score 14 (example) |
|---|---|---|
| Respiratory (PaO/FiO) | >400 | 300 (moderate ARDS) |
| Coagulation (Platelets) | >150,000 | 100,000 |
| Liver (Bilirubin) | <1.2mg/dL | 2.0mg/dL |
| Cardiovascular (MAP, vasopressors) | >70mmHg | MAP <70mmHg + norepinephrine |
| CNS (Glasgow) | 15 | 1314 (confusion) |
| Renal (Creatinine/Urine) | <1.2mg/dL | 2.0mg/dL or urine <0.5mL/kg/h |
What symptoms tip the scale from SIRS to Sepsis?
Beyond the four SIRS vitals, look for altered mental status, low urine output, a sudden drop in blood pressure, or a lactate level >2mmol/L. Those clues tell us the infection is doing damage beyond the alarm phase.
Why is early recognition crucial?
Every hour you wait to give appropriate antibiotics adds roughly a 79% increase in mortality (). In other words, time is truly tissue.
Progression Path
What is the clinical difference between Sepsis and Septic Shock?
Septic shock is sepsis plus persistent hypotension that needs vasopressors to keep a MAP 65mmHg despite adequate fluid resuscitation, often with a serum lactate 4mmol/L. Its the most dangerous rung on the ladder.
How often does SIRS progress to sepsis?
Studies suggest that 3040% of patients who meet SIRS criteria in the ED end up developing sepsis when an infection is later confirmed. The risk spikes with older age, immunosuppression, or delayed antibiotics.
What risk factors accelerate the jump?
Advanced age (65y)
Diabetes or chronic kidney disease
Immunosuppressive therapy (chemo, steroids)
Delayed source control (e.g., untreated abscess)
Understanding these can guide you to intervene sooner.
Can you prevent the progression?
Yesby acting fast. A simple 5step checklist works wonders:
- Recognize two SIRS signs + possible infection.
- Draw blood cultures before antibiotics.
- Start broadspectrum antibiotics within the first hour.
- Give 30mL/kg crystalloid bolus promptly.
- Reassess; if MAP stays <65mmHg, start norepinephrine.
Comparison Table
SIRS vs Sepsis vs Septic Shock At a Glance
| Feature | SIRS | Sepsis | Septic Shock |
|---|---|---|---|
| Trigger | Any systemic inflammation | SIRS+confirmed/suspected infection | Sepsis+refractory hypotension |
| Diagnostic criteria | 2 of 4 vitals/labs | SOFA 2 (or qSOFA2) | MAP<65mmHg after fluids + vasopressors |
| Typical labs | Temp, HR, RR, WBC | Lactate, creatinine, bilirubin, platelets | Same+pressors dose |
| Mortality (approx.) | <5% | 1030% | >40% |
| Firstline treatment | Treat underlying cause | Broadspectrum antibiotics + fluids | Same+norepinephrine additional pressors |
Diagnosis & Scoring
Which bedside tools help differentiate SIRS from Sepsis?
Quick screening with qSOFA (mental status, SBP 100mmHg, RR 22) can flag patients who likely need a full SOFA assessment. Its not perfect, but its fast and useful in the hallway.
When should you order a full SOFA score?
Whenever you suspect organ dysfunctioni.e., abnormal lactate, low urine output, or falling blood pressure. The ICU usually takes over then, but you can calculate it on the spot if you have the labs.
What lab values are most predictive?
Lactate >2mmol/L (early marker of tissue hypoxia)
Procalcitonin rises with bacterial infections, but beware of false positives in trauma.
Creactive protein useful trend, not a standalone diagnosis.
How to document the SIRS score in EMR?
Most electronic records have a template that automatically pulls temperature, heart rate, respiratory rate, and WBC. If youre using a freetext note, write something like: SIRS2/4 (Temp38.5C, HR112, RR22) pending infection workup. This makes your reasoning crystal clear.
Treatment Strategies
Is there a SIRSonly treatment plan?
When infection isnt in the picture, focus on the root cause: pain control for trauma, drainage for an abscess, steroids for severe autoimmune flares, etc. Antiinflammatories can help, but theyre not a cureall.What is the sepsis bundle and why does speed matter?
The 1hour bundle (per Surviving Sepsis Campaign) includes:
- Measure lactate.
- Obtain blood cultures before antibiotics.
- Administer broadspectrum antibiotics.
- Give 30mL/kg crystalloid bolus.
- Apply vasopressors if MAP <65mmHg after fluids.
Studies show that completing the bundle within the first hour can cut mortality by up to 20%.
How to manage fluids safely?
Start with 30mL/kg of isotonic crystalloid (normal saline or lactated Ringers). Reassess after 30minutesif the patient looks fluidoverloaded (pulmonary crackles, rising JVP) or has severe heart failure, taper or switch to a balanced solution.
When are vasopressors started?
If MAP stays below 65mmHg after the initial fluid bolus, begin norepinephrine at 0.05g/kg/min and titrate. Add epinephrine or vasopressin only if norepinephrine alone isnt enough.
Adjuncts: steroids, vitamin C, etc.?
Current evidence is mixed. Lowdose hydrocortisone (200mg/day) may help refractory shock, but its not a blanket rule. Highdose vitamin C, thiamine, and steroids (the HAT protocol) showed promise in small trials but larger RCTs are still ongoing. Always weigh the data and discuss with your team.
RealWorld Cases
Case 1 Traumatic injury SIRS only
A 27yearold motorcyclist arrived with multiple fractures. His temperature was 38.6C, HR 115, RR 24, WBC 13,000 meeting SIRS criteria. No source of infection was found. He received analgesics, surgical fixation, and fluids. Within 48hours the SIRS signs resolved without antibiotics.
Case 2 Community pneumonia Sepsis
Mrs. Patel, 68, presented with cough, fever 39C, HR 108, RR 28, WBC 14,500. Lactate was 3.2mmol/L, and her qSOFA was 2. Blood cultures were drawn, then ceftriaxone+azithromycin started within 45minutes. After 30mL/kg fluids, her MAP stayed >70mmHg, so no pressors were needed. She was discharged home after 5days, fully recovered.
Case 3 Abdominal infection Septic shock
Mr. Liu, 55, had a ruptured appendix leading to peritonitis. On arrival: Temp 39.5C, HR 138, RR 32, WBC 18,000, MAP 58mmHg despite 30mL/kg fluids, lactate 5.8mmol/L. He met sepsis criteria and quickly fell into septic shock. Norepinephrine was started, source control via emergent surgery, and broadspectrum antibiotics (piperacillintazobactam) administered. After 72hours in ICU, his SOFA score fell from 12 to 4, and he was weaned off pressors.
What clinicians learned from these cases
Not every SIRS episode needs antibioticstreat the cause.
Early lactate measurement can tip the scales toward sepsis.
Prompt source control (surgery, drainage) is as vital as fluids and meds.
Continuous reassessment prevents overtreatment and saves lives.
Bottom Line
In a nutshell, sirs vs sepsis is a matter of alarm versus alarm+infection. SIRS is the bodys warning light; sepsis is that warning paired with a proven or suspected infection, and septic shock is the point where the warning light turns into a fullblown emergency. Spotting the shift early, applying the 1hour bundle, and staying vigilant about organ function can dramatically improve outcomes.
If you ever notice two or more of the classic SIRS signs (fever, rapid heartbeat, fast breathing, or an abnormal whitebloodcell count) and suspect an infection, dont waitcall your healthcare provider and let them know what youre seeing. Early action can be the difference between a quick recovery and a serious ICU stay.
Whats your experience with these warning signs? Have you ever helped a loved one navigate a sepsis scare? Share your story in the comments below, or drop any questions you haveI\'m here to help!
FAQs
What is the main difference between SIRS and sepsis?
SIRS is a systemic inflammatory response that can be caused by infection, trauma, or other insults, whereas sepsis is SIRS plus a confirmed or suspected infection that leads to organ dysfunction.
How many SIRS criteria must be met to consider the diagnosis?
At least two of the four classic criteria—temperature, heart rate, respiratory rate (or PaCO₂), and white‑blood‑cell count—must be present.
When should the SOFA score be used instead of SIRS?
The SOFA score is used when infection is suspected and you need to assess organ dysfunction; an increase of ≥2 points indicates sepsis under the Sepsis‑3 definition.
What are the first‑hour actions for a patient with suspected sepsis?
Measure lactate, obtain blood cultures before antibiotics, start broad‑spectrum antibiotics, give 30 mL/kg crystalloid, and initiate vasopressors if MAP remains <65 mm Hg after fluids.
Can SIRS progress to septic shock without treatment?
Yes. If the underlying infection isn’t controlled and hypotension persists despite fluid resuscitation, the patient can quickly move from sepsis to septic shock, which carries >40 % mortality.