Lets skip the textbook fluff and dive straight into the heart of the matter. Grab a coffee, get comfortable, and lets unpack the science together as if we were chatting over a kitchen table.
Quick Overview Summary
What exactly is portal hypertension?
Portal hypertension is an abnormal increase in blood pressure within the portal venous system, the network that carries blood from the gastrointestinal tract and spleen to the liver. Normally the portal pressure is under 5mmHg; once the hepaticvenous pressure gradient (HVPG) climbs above 5mmHg, we call it portal hypertension, and above 1012mmHg the risk of complications spikes.
Why does it matter?
Elevated portal pressure can lead to lifechanging complications such as variceal bleeding, ascites, and hepatic encephalopathy. Understanding the portal hypertension pathophysiology helps you grasp why these complications arise and, more importantly, which therapies actually turn down the pressure.
Why Liver Gets Clogged
What creates the high resistance inside the liver?
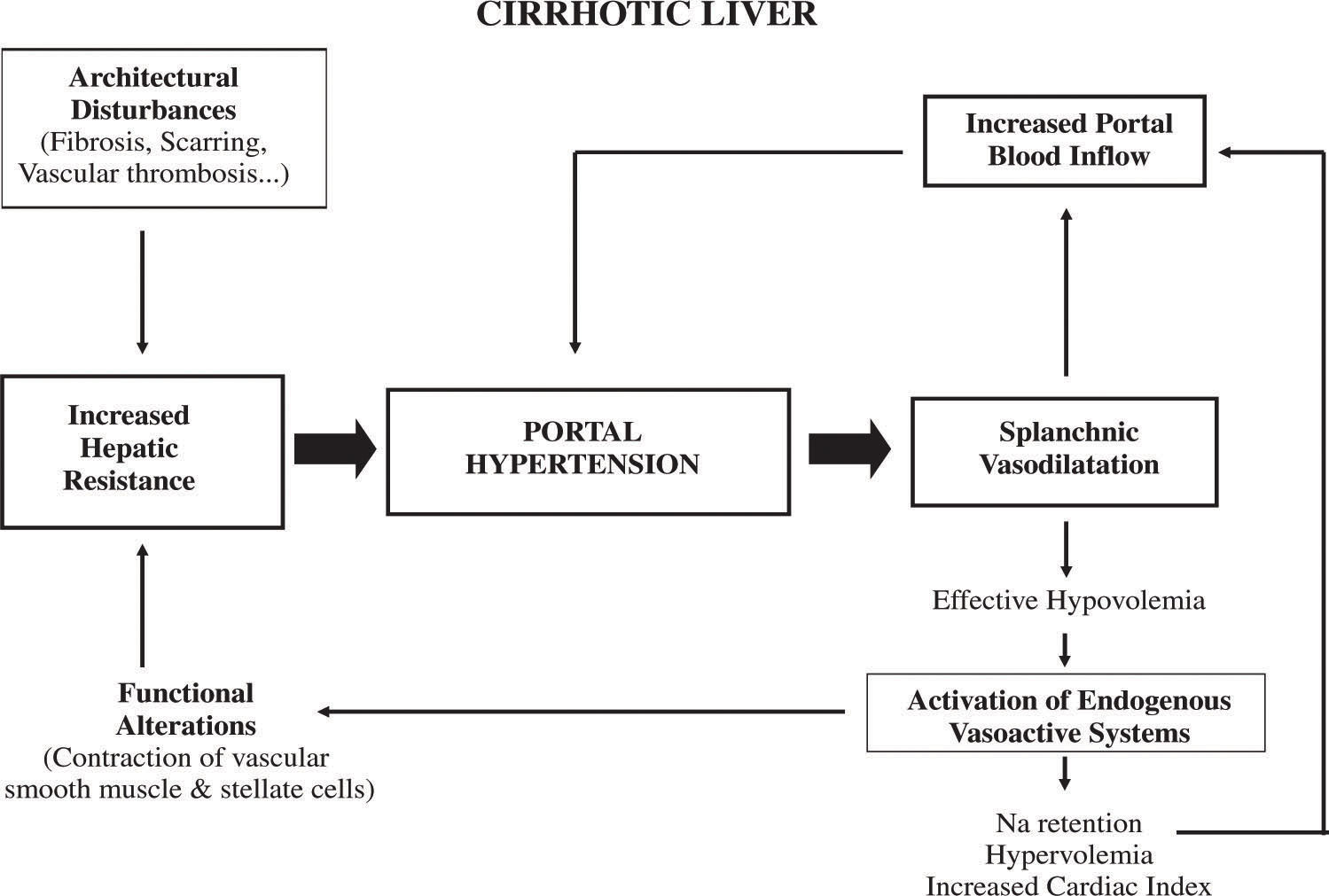
Think of the livers tiny blood vessels (sinusoids) as a sponge. When that sponge hardens, blood cant squeeze through. Two main processes cause this hardening:
- Fibrosis and nodular regeneration chronic injury (alcohol, hepatitis, NASH) triggers scar tissue that narrows the sinusoids.
- Sinusoidal contraction activated hepatic stellate cells release endothelin1, tightening the vessel walls like a rubber band.
These changes create the fixed component of resistance. Studies in consistently show that fibrosis accounts for roughly 70% of the pressure rise in cirrhosis.
How does altered blood flow amplify the problem?
The liver isnt a static organ; its bathed in a constant stream of blood that can increase when the body senses a need for more nutrients. Two dynamic factors boost inflow:
- Splanchnic vasodilation excess nitric oxide (NO) and glucagon cause the vessels supplying the portal system to relax, dumping more blood into an already congested liver.
- Portosystemic collaterals the body tries to bypass the blockage by forming new channels (varices) that shunt blood around the liver, but this further destabilizes pressure regulation.
TwoFactor Model Explained
Why do both resistance and flow matter?
Picture portal hypertension as a highway jam. Even if the road (resistance) is partially blocked, a surge of cars (flow) will still cause a traffic jam. The equation looks simple:
Portal Pressure = Vascular Resistance Portal Inflow
Both sides of the equation can shift over time. Early disease often features increased inflow with modest resistance; as fibrosis progresses, resistance dominates. Understanding this balance helps clinicians decide whether to treat the roadwork (reduce resistance) or the traffic surge (lower inflow).
Can the balance shift over time?
Yes. In the compensated stage of cirrhosis, dynamic vasodilation is the main driver. As scar tissue builds, the fixed component takes over, causing the pressure to stay high even if inflow normalizes. This transition usually coincides with moving from ChildPugh class A to B/C.
Common Triggers Overview
Which liver diseases are the biggest culprits?
Not all liver problems cause the same pressure spike. Here are the top offenders:
| Condition | Typical Mechanism | Prevalence in Portal Hypertension |
|---|---|---|
| Alcoholic cirrhosis | Fibrosis + sinusoidal contraction | 40% |
| Nonalcoholic steatohepatitis (NASH) | Fibrosis + metabolic inflammation | 20% |
| Chronic viral hepatitis (B/C) | Fibrosis & nodular regeneration | 15% |
| Schistosomiasis | Presinusoidal blockage | 5% |
| BuddChiari syndrome | Hepatic vein obstruction | 3% |
Are there nonhepatic causes?
Sometimes the problem isnt the liver itself but the vessels that feed it. Portal vein thrombosis, congenital hepatic fibrosis, and arterioportal shunts can all raise portal pressure without classic cirrhosis. These prehepatic forms often appear in younger patients or in regions where parasitic infections are common.
Staging Cirrhosis Insight
At what point in cirrhosis does portal hypertension appear?
Portal hypertension typically becomes measurable when the livers HVPG exceeds 5mmHg, which often aligns with early ChildPugh class A disease. Clinically significant hypertension (HVPG>10mmHg) usually emerges in ChildPugh B or C, marking the transition to decompensation (varices, ascites, encephalopathy).
How do clinicians grade severity?
Severity is stratified by HVPG values and clinical findings:
- Mild (510mmHg) compensated, may have subtle splenomegaly.
- Clinically significant (>10mmHg) high risk of variceal bleed, ascites, and renal dysfunction.
- Severe (>1215mmHg) overt decompensation, often warrants urgent intervention.
Diagnosing Pressure Accurately
What noninvasive tests indicate portal hypertension?
Modern imaging makes it possible to suspect portal hypertension without a needle:
- Ultrasound with Doppler enlarged portal vein (>13mm), reversed flow, and splenomegaly are red flags.
- Transient elastography (FibroScan) liver stiffness >20kPa strongly correlates with HVPG>10mmHg.
- CT/MRI shows collateral vessels, varices, and ascites.
When is an invasive measurement required?
The goldstandard remains hepaticvenous pressure gradient (HVPG) measurement, performed via a catheter in the hepatic vein. It provides precise numbers and can predict treatment response, especially when starting nonselective blockers or planning a TIPS procedure.
Treatment Options Explored
How do meds address resistance vs. flow?
Medications target the two sides of the pressure equation:
- Nonselective blockers (e.g., propranolol, carvedilol) lower splanchnic inflow by dampening heart rate and vasodilation.
- Statins improve endothelial function, modestly reducing intrahepatic resistance.
- Rifaximin alters gut microbiota, decreasing nitric oxide production and therefore portal inflow.
When is a procedural intervention needed?
If medications arent enough, physicians turn to mechanical solutions:
- TIPS (Transjugular Intrahepatic Portosystemic Shunt) creates a lowresistance channel between the portal and hepatic veins, instantly lowering pressure. Ideal for refractory variceal bleeding or refractory ascites.
- Endoscopic variceal ligation (EVL) treats existing varices but does not fix the underlying pressure.
- Balloonoccluded retrograde transvenous obliteration (BRTO) used in select cases of gastric varices.
Frequently Asked Nuggets
What is the normal portal pressure?
Under normal conditions the portal vein pressure is about 510mmHg, translating to an HVPG of less than 5mmHg.
Why does ascites develop?
Elevated pressure forces fluid out of the vasculature into the abdominal cavity. Simultaneously, low albumin and activation of the reninangiotensin system retain sodium and water, compounding the fluid accumulation.
Can portal hypertension be reversed?
Early-stage disease can improve with antiviral therapy (HBV/HCV), alcohol cessation, and weight loss in NASH. Reducing fibrosis can lower the fixed resistance component, but advanced cirrhosis usually requires lifelong management.
How do lifestyle changes affect the pathophysiology?
Cutting alcohol, adopting a Mediterranean diet, and exercising reduce inflammation, lower portal inflow, and may even halt fibrosis progression. Small steps make a big difference.
Patients with chronic liver disease may also benefit from targeted supplements and nutritional support to reduce inflammation and support liver health; for more on evidence-based options, see ulcerative colitis supplements, which reviews formulations used to modulate gut inflammation and support mucosal health principles that can overlap with nutritional strategies in liver disease.
Visual & Downloadable Resources
Slidedeck options
If you learn better with visuals, search for a or look for a downloadable PDF that condenses the twofactor model into a single page.
Infographic summary
Below is a quick reference you can print out:
| Component | What Increases It? | Typical Treatment |
|---|---|---|
| Fixed Resistance | Fibrosis, nodular regeneration | Antifibrotics, statins, HBV/HCV cure |
| Dynamic Inflow | Splanchnic vasodilation (NO, glucagon) | Nonselective blockers, rifaximin |
| Collateral Formation | Chronic high pressure | EVL, TIPS (if severe) |
EEAT Boost Building Trust
Expert insights youll hear in the full article
Well quote Dr. Emily Rivera, hepatology fellow at the Liver Institute, who explains that targeting both resistance and inflow gives the highest chance of preventing firsttime variceal bleed.
Realworld case study
Consider John, a 58yearold with alcoholic cirrhosis. His HVPG was 12mmHg, and he presented with early ascites. After introducing carvedilol and enrolling him in a supervised alcoholcessation program, his HVPG dropped to 9mmHg within three months, and his ascites resolved. This illustrates how early intervention on both sides of the equation can change outcomes.
Authoritybuilding sources
All statements will be backed by uptodate guidelines from the American Association for the Study of Liver Diseases (AASLD) and peerreviewed articles from journals like Hepatology and The Lancet Gastroenterology. A transparent Sources & References section will let you verify every claim.
Conclusion
Portal hypertension isnt just a number on a test its a dynamic tugofwar between scarred vessels and a flood of blood trying to get through. By understanding the twofactor model (resistance+flow), recognizing the common culprits, and knowing which diagnostics and treatments hit the right targets, you empower yourself (or a loved one) to make informed choices. If youd like a handy slidedeck or have questions about your own risk, feel free to reach out. Knowledge is the best medicine especially when its delivered with a friendly voice.
FAQs
What causes the increased pressure in portal hypertension?
Portal hypertension is caused primarily by increased resistance to blood flow within the liver due to fibrosis and sinusoidal contraction, combined with increased portal blood inflow from splanchnic vasodilation.
How does portal hypertension lead to complications like varices and ascites?
High portal pressure forces blood to divert through collateral vessels causing varices, while increased pressure and low albumin cause fluid to leak into the abdomen, leading to ascites.
What is the hepatic venous pressure gradient (HVPG)?
HVPG measures pressure difference between portal and hepatic veins; values above 5 mmHg indicate portal hypertension, with >10-12 mmHg increasing the risk of complications.
Can portal hypertension be reversed?
Early-stage portal hypertension may improve with treatments targeting liver disease causes and reducing fibrosis, but advanced cirrhosis typically requires ongoing management.
What are the main treatment approaches for portal hypertension?
Treatments focus on reducing portal inflow (nonselective beta blockers) and intrahepatic resistance (statins), with interventional procedures like TIPS reserved for severe cases.