Imagine youre sitting in a coffee shop, and a friend confides that their throbbing head feels like a drill. You want to help, but the right question is: can a quick neurological exam tell you whether its a migraine or something more serious? In the next few minutes Ill walk you through exactly thatstep by step, with realworld tips, redflag alerts, and a handy cheatsheet you can actually use in the clinic.
Why the Exam Matters
A good history is priceless, but the neurological exam is the shortcut that can catch dangerous problems before they slip through the cracks. Its the difference between sending someone home with a simple analgesic and ordering an urgent CT scan that saves a life.
What does the exam reveal that history cant?
History tells you what the headache feels like; the exam shows you how the brain is functioning right now. A normal exam often points to primary headaches (like migraine or tensiontype), while focal deficitslike a drooping eyelidraise the alarm for secondary causes.
How does it fit into the headache workup algorithm?
The starts with history, then the neurological exam, then redflag screening, and finally imaging if needed. Skipping the exam is like trying to bake a cake without checking if the ovens on.
Which redflag findings should make you pause?
Think of the classic SNOOP mnemonicSystemic symptoms, New onset, Older age, Onset sudden, Progressive. When you pair SNOOP with any abnormal neuro sign (e.g., papilledema), youve got a green light for immediate imaging.
Quick RedFlag Comparison
| RedFlag | Neuro Sign | Suggested Action |
|---|---|---|
| Sudden, worst headache | Absent papilledema, normal cranial nerves | Urgent noncontrast CT |
| Age>50 with new headache | Focal weakness or asymmetric reflexes | MRI with contrast |
| Systemic illness (fever, weight loss) | Neck stiffness or altered mental status | CT/MRI + lumbar puncture if indicated |
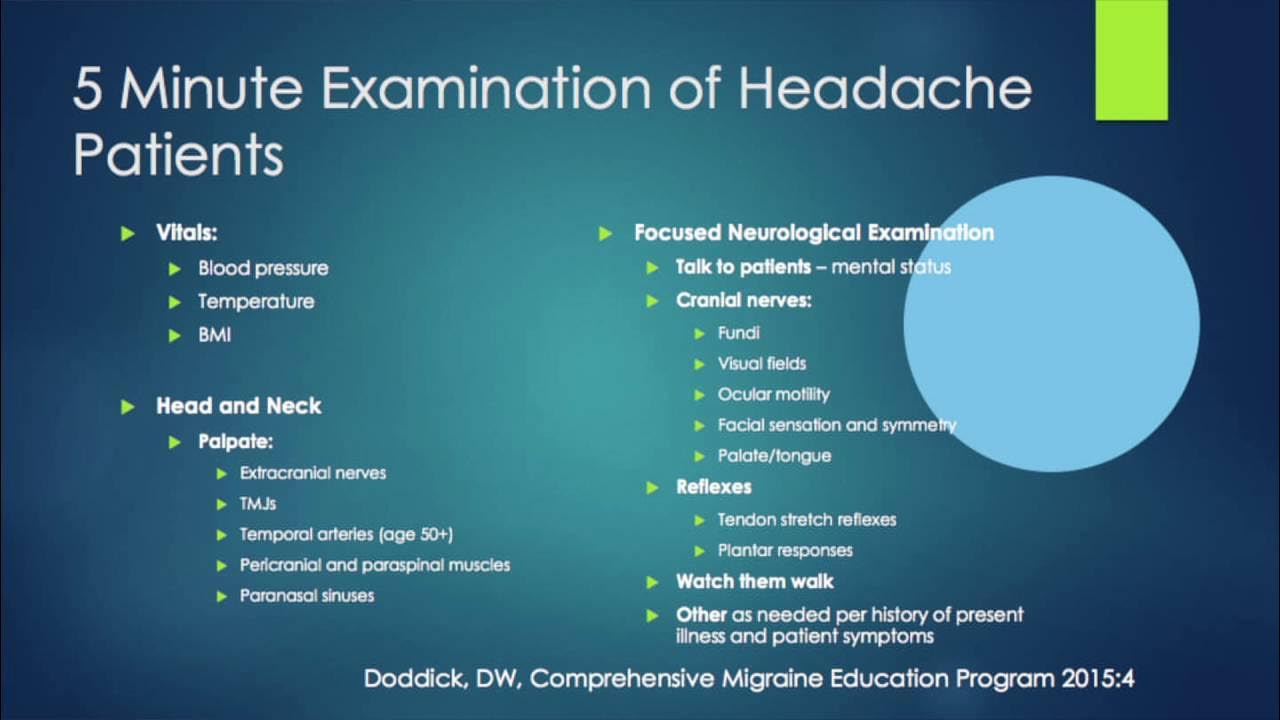
EightStep Exam
Heres the core of what many call the Eight Basic Steps. Think of it as a checklist you can run through in under five minuteseven during a busy clinic.
1. Mental Status
Ask simple orientation questions (Whats todays date?). A clear, alert mind usually steers you toward primary headaches. Confusion? Thats a red flag.
2. Cranial Nerves IXII
Check vision, pupil reactions, facial symmetry, hearing, and tongue movement. For instance, a sluggish pupillary response can hint at increased intracranial pressure.
3. Motor Strength
Rate each limb on a 05 scale. Any asymmetrylike 4/5 on one armshould make you think about a focal lesion.
4. Sensory Exam
Light touch and pinprick across both sides. Do you feel this on both arms? Uneven sensation can be a clue to a brainstem or spinal problem.
5. Coordination & Gait
Fingertonose, heeltoshin, and a quick walk. Unsteady gait may point to cerebellar involvementsomething youd never catch from history alone.
6. Reflexes
Deep tendon reflexes and plantar response. Hyperreflexia or a Babinski sign is a classic upper motor neuron finding.
7. Cerebellar Signs
Romberg test (standing with eyes closed). A positive Romberg suggests dorsal column pathologynot a typical migraine.
8. Head & Neck Inspection
Look for scalp tenderness, sinus tenderness, or neck stiffness. Temporal artery tenderness could be giant cell arteritisa real emergency.
MiniChecklist (PrintFriendly)
Download a printable PDF of this eightstep exam and keep it on your exam room wall.
Red Flag Checklist
Even a perfect exam can miss a hidden danger if you forget the redflag questions. Heres a condensed list you can ask on the spot.
What are the key headache assessment questions?
Alongside SNOOP, ask:
- Did the pain start suddenly or build up?
- Any recent head trauma or surgery?
- Do you have fever, neck stiffness, or visual changes?
- Are you on any new medications?
How do specific neuro signs change management?
Finding papilledema = immediate CT/MRI. New focal weakness = MRI with contrast. Normal exam + benign history = reassure and treat symptomatically.
RedFlag Decision Tree
| RedFlag Question | Abnormal Neuro Sign? | Imaging Recommendation |
|---|---|---|
| Sudden onset (worst ever)? | Yes focal deficits | Urgent noncontrast CT |
| Age>50 with new headache? | Yes papilledema | MRI with contrast |
| Systemic illness (fever, weight loss)? | Yes neck stiffness | CT + possible LP |
Workup Algorithm
Lets stitch the pieces together. Imagine a flowchart in your mind: History Headache HPI template Neurological exam Redflag assessment Imaging or discharge.
What does a good HPI template look like?
Use a structured that captures onset, location, quality, severity, duration, and associated symptoms (the OLDCARTS of headaches). Add a line for Neuro exam findings so you dont forget to document them.
How to integrate the algorithm into an EMR?
Many EMRs let you embed a dropdown for Neurological exam normal/abnormal that automatically flags the patient for imaging if you select abnormal. Its a tiny tweak that saves a lot of time.
Sample Flowchart (Text Version)
- Patient presents with headache.
- Complete HPI using the headache HPI template.
- Perform the eightstep neurological exam.
- Ask redflag questions (SNOOP + extra).
- If any red flag or abnormal neuro sign Order imaging per algorithm.
- If all normal Reassure, treat symptomatically, schedule followup.
Migraine vs. TensionType vs. Secondary
Not all headaches are created equal. Heres a quick compareandcontrast of what youll typically see on exam.
What does a normal exam look like in classic migraine?
Most migraine patients have a completely normal neuro exam. You might notice photophobia or phonophobia, but motor strength, cranial nerves, and reflexes remain intact.
When do you suspect a secondary headache?
Any focal deficit, abnormal gait, or papilledema instantly pushes you into the secondary category. Even subtle signs like a slight facial droop deserve a second look.
Exam Findings by Headache Type
| Headache Type | Typical Neuro Findings |
|---|---|
| Migraine | Completely normal; possible mild photophobia |
| Tensiontype | Normal exam; may have neck muscle tenderness |
| Cluster | Possible Lacrimation, nasal congestion, but neuro exam normal |
| Secondary (e.g., bleed, tumour) | Focal weakness, papilledema, altered mental status |
OSCE & Clinical Skills Tips
If youve ever faced the dreaded headache physical exam OSCE station, you know the pressure. Here are a few tricks that helped me (and many geeky medics) ace it.
What are the most common OSCE pitfalls?
Skipping the cranial nerve exam, rushing through the gait assessment, or forgetting to mention your findings in the assessment part of the station. Remember: the examiner wants to see a systematic, reproducible approach.
How can you finish the exam in under three minutes?
Start with mental status (30seconds), then run through cranial nerves (45seconds), quickly assess motor strength (30seconds), and finish with a heeltoe walk (45seconds). Practicing with a timer makes the process feel natural.
OSCE QuickDos & Donts
- Do maintain eye contact while testing pupils.
- Do explain each maneuver (Ill now tap your knee) to keep the patient comfortable.
- Dont skip the reflexeseven if you think theyre normal.
- Dont rush the gait; a brief walk tells you a lot.
Documentation & Patient Talk
Great exams are useless if you cant document them clearly or explain them to the patient without scaring them.
How to write a concise neuroexam note?
Use the SOAP format: Subjective (headache description), Objective (neuro exam findings), Assessment (primary vs. secondary suspicion), Plan (imaging or reassurance). A bulletpoint list for each cranial nerve can be lifesaver.
How to reassure a patient with a normal exam?
Say something like, Your exam looks completely normal, which is what we see in common migraine. Well treat the pain and keep an eye on any new symptoms, but theres no sign of anything dangerous right now. Using plain language builds trust.
Sample Note Excerpt
O:- 28yo female, throbbing left temporal headache 3days, photophobia, no nausea.A:- Neurological exam: Alert, oriented 3; CN IIXII intact; 5/5 strength all limbs; normal reflexes; gait steady; no papilledema.P:- Likely migraine; prescribe NSAID + triptan; advise redflag symptoms; followup in 2weeks.
Quick FAQs (FeaturedSnippet Ready)
Can a normal neurological exam rule out a brain tumour?
A normal exam makes a tumour less likely, but it doesnt absolutely rule it outespecially if symptoms are atypical. Imaging is still considered if redflag criteria are present.
When should I order an MRI after a headache exam?
Order MRI when you have any focal deficit, papilledema, newonset headache after age50, or systemic symptoms like fever. MRI is more sensitive for softtissue lesions than CT. For help navigating insurance coverage or patient assistance programs that sometimes affect access to advanced therapies, consider resources like Exondys 51 insurance which outline common coverage questions and pathways.
What are the most common neuroexam mistakes in primary care?
Skipping the cranial nerve assessment, not checking reflex symmetry, and forgetting to document gait. A quick mental checklist (the eightstep exam) helps avoid these lapses.
Conclusion
Got this far? Awesomeyou now have a solid, eightstep neurological exam, a redflag checklist, and a workflow that fits right into the headache workup algorithm. Remember, a thorough exam is the fastest gatekeeper between a harmless migraine and a lifethreatening bleed. Grab the printable cheatsheet, practice the OSCE tricks, and keep the HPI template handy. Your patients will thank you for the confidence you bring to every headache visit.
Whats your favorite tip for speeding up a neuro exam? Share your story in the comments, or download the and let us know how it works for you. If you have any lingering questions, feel free to askI\'m here to help!
FAQs
When should I perform a neurological exam for a patient with headache?
A neurological exam is essential for any new, worsening, or atypical headache, especially if red‑flag symptoms are present or the patient is over 50.
What red‑flag findings on the exam require immediate imaging?
Abnormal papilledema, focal motor weakness, asymmetric reflexes, new cranial nerve deficits, or an altered level of consciousness all mandate urgent CT or MRI.
Can a completely normal neurological exam rule out a brain tumour?
A normal exam makes a tumour less likely but does not absolutely exclude it; imaging is still warranted if red‑flag criteria are met.
How much time does the eight‑step neurological exam usually take in a busy clinic?
With practice you can complete the eight steps in under three minutes while still maintaining a systematic approach.
What is the best way to document the exam in an EMR?
Use a concise SOAP note with bullet‑point entries for each cranial nerve and a brief statement of motor, sensory, reflex, and gait findings.