Ever walked into a clinic with a pounding head and left wondering if youd need a CT scan, a prescription, or just a cup of tea? Youre not alone. The American Academy of Family Physicians (AAFP) has put together a straightforward, evidencebased roadmap that helps primarycare cliniciansand anyone whos curiousfigure out whats really going on, when to worry, and how to get relief fast. Lets break it down together, step by step, with a friendly tone that feels more like a chat over coffee than a textbook.
Why This Guide Matters
Headaches are one of the most common reasons people visit a doctor, yet many of us treat them as just a headache. The problem? Some headaches hide serious conditions, while others are harmless but disruptive. The give us a clear, nofluff approach to separate the two, so you can avoid unnecessary tests and get the right care quickly.
Workup Algorithm
StepbyStep Flowchart
Step1: Quick History Ask who, what, when, and how bad. A few targeted questions often reveal the type of headache.
Step2: Focused Physical Exam A brief neuro check, eye exam, and sinus palpation are usually enough.
Step3: RedFlag Checklist (SNOOP) If anything on this list pops up, its time for imaging or urgent referral.
Step4: PrimaryHeadache Classification Decide whether its tensiontype, migraine, or cluster, then move to treatment.
Printable Algorithm (PDF)
Download the for a handy visual reference you can keep on your desk.
Mastering the History
Typical vs. Atypical Features
What does the pain feel like? Is it a tight band around your head (classic tensiontype) or a throbbing, unilateral hammer (maybe migraine or cluster)? Do you have nausea, light sensitivity, or visual aura? Any recent head trauma, fever, or new medication?
Example History Worksheet
| Question | Why It Matters |
|---|---|
| Onset? | Sudden thunderclap suggests subarachnoid bleed. |
| Location? | Unilateral pounding points to migraine/cluster. |
| Associated symptoms? | Nausea, photophobia = migraine; nasal congestion = sinus. |
| Triggers? | Stress = tension; certain foods = migraine. |
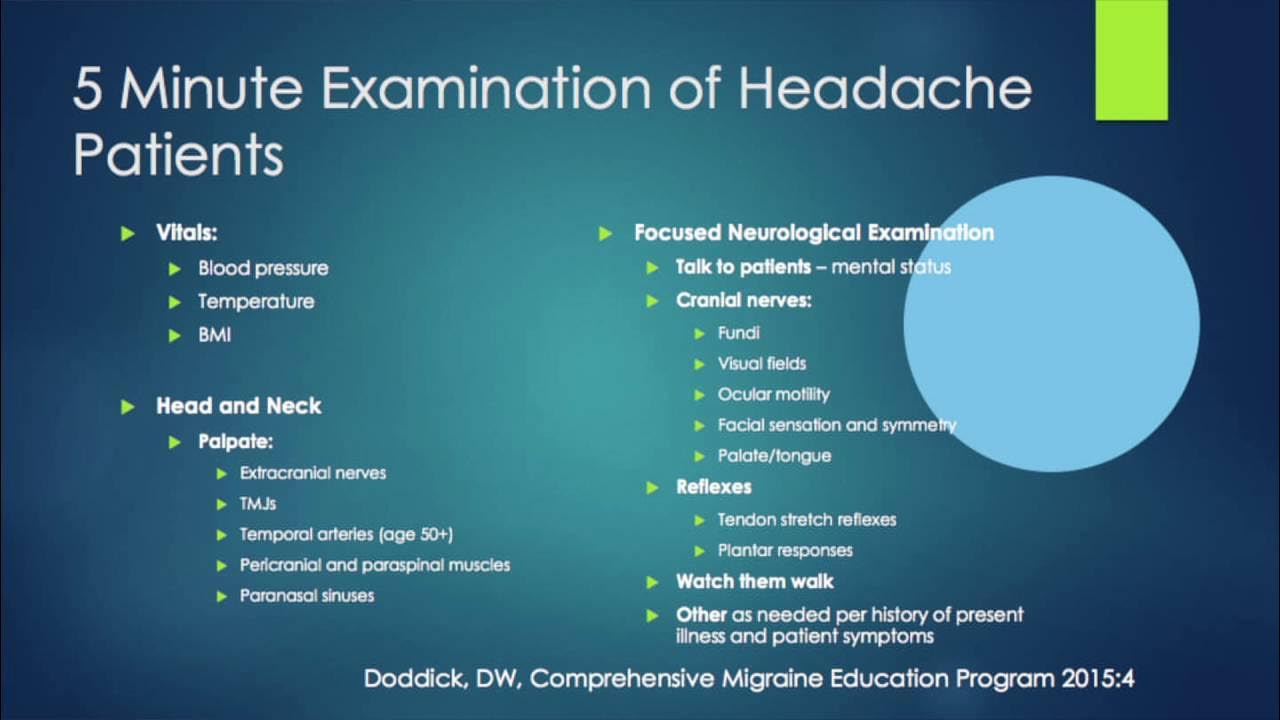
Physical Exam Essentials
NeuroCheck Highlights
A quick cranial nerve screen (IIXII) catches focal deficits. Dont forget to look at the back of the eyes for papilledemaan important red flag for increased intracranial pressure.
Findings Comparison
| Finding | Primary Headache | Secondary Concern |
|---|---|---|
| Papilledema | No | Yes consider mass lesion. |
| Focal weakness | No | Yes stroke, tumor. |
| Sinus tenderness | No | Possible sinusitis. |
RedFlag Symptoms
SNOOP Revisited
- Systemic symptoms (fever, weight loss)
- Neurologic signs (weakness, confusion)
- Onset sudden or thunderclap
- Older age at onset (50)
- Previous pattern change
If any of these appear, order appropriate imagingCT if you suspect bleed, MRI for tumors, or lumbar puncture for meningitis.
Decision Tree for Imaging
| Red Flag | Recommended Test |
|---|---|
| Thunderclap onset | CT head noncontrast |
| Focal neurologic deficit | MRI brain with contrast |
| Fever + neck stiffness | LP after CT |
| Age50 with new headache | CT or MRI based on other signs |
Primary Headache Types
TensionType (AAFP 2018)
Imagine a tight band squeezing your skullno nausea, no light sensitivity, just a dull, constant ache. The 2018 tension headache treatment guidelines suggest starting with NSAIDs (ibuprofen 400600mg) or acetaminophen, then moving to lowdose amitriptyline if it becomes chronic.
Migraine (AAFP Migraine Prophylaxis)
Migraine feels like a pulsing hammer, often on one side, and invites nausea, photophobia, and sometimes an aura. Acute relief usually begins with NSAIDs or acetaminophen, then triptans if the pain persists. For frequent attacks, the AAFP migraine prophylaxis recommends betablockers (propranolol), topiramate, or newer CGRP antagonists.
Cluster Headache (AAFP Cluster Overview)
These are the alarm clocks of headachesshort, excruciating, unilateral pain with tearing or nasal stuffiness. The firstline rescue is 100% oxygen for 15 minutes or a subcutaneous sumatriptan injection. Preventive therapy often includes verapamil.
Headache Type Comparison
| Feature | Tension | Migraine | Cluster |
|---|---|---|---|
| Onset | Gradual | Gradual to sudden | Sudden |
| Location | Bilateral band | Unilateral | Unilateral |
| Associated Signs | None | Nausea, photophobia | Tearing, nasal congestion |
| Firstline Acute Rx | NSAID | Triptan | Oxygen / Sumatriptan |
Secondary Headache Workup
Common Causes in Primary Care
Even if the pain looks normal, it could be sinusitis, medication overuse, temporal arteritis, or something more serious like an intracranial mass. Treating the underlying causewhether its switching a medication or starting steroids for arteritisoften resolves the headache.
Labs & Imaging Quick Reference
| Condition | Lab Test | Imaging |
|---|---|---|
| Temporal arteritis | ESR, CRP | Temporal artery ultrasound |
| Medication overuse | None | None (clinical) |
| Sinusitis | CBC if fever | CT sinuses if chronic |
| Intracranial mass | None | MRI brain |
EvidenceBased Treatment Pathways
Acute Management Algorithms
For tensiontype, start with an NSAID. If pain persists after 23 days, consider adding a lowdose tricyclic antidepressant for prophylaxis. Migraine attacks respond well to triptans, but if you have cardiovascular risk, use a gepant instead. Cluster headaches demand rapid oxygen therapythink of it as an instant reset button.
Prophylaxis Decision Tree (AAFP Migraine Prophylaxis 2025)
- Headaches >4days/month? Start prophylaxis.
- Firstline: Propranolol (if no asthma), topiramate, or CGRP monoclonal.
- Assess sideeffects after 4weeks, then adjust dose.
Sample Prescription Table
| Drug | Starting Dose | Goal Dose | Key Contraindications |
|---|---|---|---|
| Propranolol | 40mg BID | 160mg/day | Asthma, bradycardia |
| Topiramate | 25mg nightly | 100mg/day | Kidney stones, cognitive fog |
| Amitriptyline | 10mg HS | 50mg HS | Heart block, glaucoma |
Putting It All Together: A RealWorld Case
Emilys Story
Emily, a 34yearold graphic designer, came in with a daily tightband headache that lastedhours and got worse after long screen sessions. Her history was classic for tensiontype: no nausea, no visual aura, and the pain improved with ibuprofen. On exam, neuro was normal, and there were no redflags. Following the AAFP workup algorithm, we started ibuprofen400mgTID and advised ergonomic breaks. After three weeks, her headaches persisted, so we added lowdose amitriptyline25mg at night.
Two months later, Emily reports a 70% reduction in pain frequency. She also learned stressmanagement techniquessomething the AAFP emphasizes as part of a holistic approach. This story illustrates how the algorithm, combined with personalized care, can turn a just another headache into a manageable condition.
Frequently Asked Questions (Quick Snippets)
What does headache AAFP actually refer to?
Its the set of evidencebased guidelines from the American Academy of Family Physicians that outline how to assess, diagnose, and treat common headaches in primary care.
Can OTC meds cure a migraine?
Overthecounter NSAIDs can help mild attacks, but most migraines need a triptan or newer CGRP medication for reliable relief.
When is a CT scan truly necessary?
Whenever a redflag symptom from the SNOOP list appearssudden onset, neurologic deficit, fever, or new headache after age50a CT (or MRI) is warranted.
How often should I see a specialist?
If headaches are frequent (>4days/month), disabling, or refractory to primarycare treatment, a referral to a neurologist is recommended.
Resources & Downloadables
For those who love a good cheatsheet, grab the . It condenses the entire workup algorithm, redflag checklist, and treatment ladder onto a single page you can keep in your pocket.
Also, consider printing the Headache Differential Diagnosis table to hang in your office or home office. Seeing the options sidebyside makes it easier to spot patterns and decide when to act.
Conclusion
Headaches dont have to be a mystery, and they certainly dont have to dominate your life. By using the AAFP guidelinesquick history, focused exam, the SNOOP redflag safety net, and evidencebased treatmentyou can identify whether a headache is benign or a signal for urgent care, and you can start the right therapy right away. Remember, understanding both the benefits and the risks of each approach is the key to balanced, trustworthy care.
If you found this guide helpful, why not share it with a friend whos been battling that stubborn bandlike ache? And if you have a headache story of your ownwhether its a triumph or a puzzling casefeel free to reach out. Together we can turn headaches from just another symptom into something we manage confidently and compassionately.
FAQs
What does headache AAFP actually refer to?
Its the set of evidence-based guidelines from the American Academy of Family Physicians that outline how to assess, diagnose, and treat common headaches in primary care.[1]
When is a CT scan truly necessary for headache?
Whenever a red flag symptom from the SNOOP list appears—sudden onset, neurologic deficit, fever, or new headache after age 50—a CT (or MRI) is warranted.[5][7]
Can OTC meds cure a migraine?
Over-the-counter NSAIDs can help mild attacks, but most migraines need a triptan or newer CGRP medication for reliable relief.[3]
How often should I see a specialist for headaches?
If headaches are frequent (>4 days/month), disabling, or refractory to primary care treatment, a referral to a neurologist is recommended.[2]
What are first-line treatments for tension-type headaches?
For tension-type headaches, start with NSAIDs like ibuprofen 400-600 mg or acetaminophen, then low-dose amitriptyline if chronic.[1]