If you or someone you love is living with Alzheimers, you might notice moments that feel like a blank stare or a sudden, brief shaking. Those episodes can be seizures, and theyre more common than many people realize. In this article well unpack what Alzheimers seizures are, why they happen, how to spot them early, what treatments exist, and what the overall outlook looks like. Lets dive inno fluff, just the info you need to feel empowered.
What Are Seizures?
Definition and Types
Seizures are bursts of abnormal electrical activity in the brain. In Alzheimers they can show up as focal onset events (affecting just one part of the brain) or as generalized seizures (involving the whole brain). Even silent seizuresthose without obvious shakingcan interrupt brain function for seconds at a time.
How They Differ from Classic Epilepsy
Epilepsy is a chronic condition where seizures recur without an obvious trigger. Alzheimers-related seizures, on the other hand, stem from the brains gradual degeneration. While the electrical storm looks similar on an EEG, the underlying cause is the amyloid plaques and tau tangles that characterize Alzheimers disease.
How Common?
Prevalence Rates
Studies estimate that between 10% and 64% of people with Alzheimers will experience at least one seizure during the course of their illness. The wide range reflects differences in study methods, but the consensus is clear: seizures are far from rare in dementia.
Comparison with Other Dementias
Vascular dementia carries a slightly higher risk of seizures because of the added impact of small-vessel disease, while Lewy-body dementia shows a lower incidence. Understanding these nuances helps clinicians personalize monitoring strategies.
Seizure Prevalence by Dementia Type
| Dementia Type | Seizure Prevalence | Key Notes |
|---|---|---|
| Alzheimers disease | 10-64% | Risk rises with disease progression |
| Vascular dementia | 15-70% | Often linked to cerebrovascular lesions |
| Lewy-body dementia | 5-20% | Usually focal-onset |
Why Do They Occur?
NeuroDegenerative Changes
Alzheimers pathology creates a hyperexcitable environment. Amyloid plaques interfere with neuronal communication, while tau tangles destabilize the cells that keep electrical signals in check. The result? Neurons fire off randomly, producing seizures.
Vascular Contributions
Many Alzheimers patients also have small-vessel disease. Tiny strokes or chronic low-grade ischemia damage the brains circuit board, making it more prone to electrical misfires. This overlap explains why clinicians often discuss vascular health as part of seizure risk.
Sleep Disruption
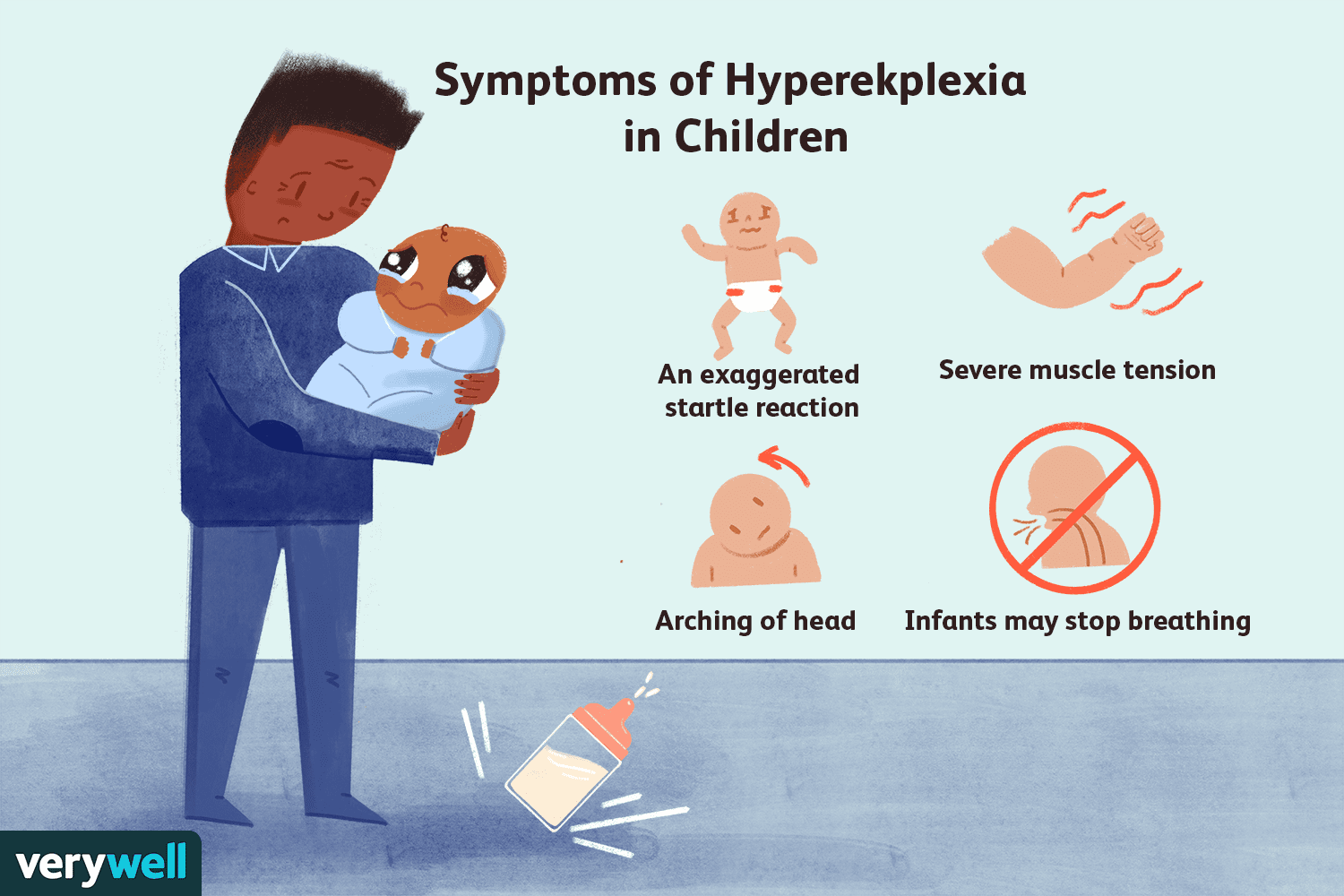
Sleep is the brains nightly reset button. When Alzheimers patients experience fragmented sleep, the nighttime EEG frequently shows epileptiform spikestiny warning signs that a seizure could erupt the next day. Notably, certain neurological conditions like atypical Rett syndrome can also feature both seizures and sleep disturbances, highlighting how brain disorders often have overlapping symptoms and risks.
When Do They Appear?
Early-Stage Seizures
Surprisingly, seizures can surface before memory loss becomes obvious. These silent seizures may manifest as brief moments of confusion or a sudden stare that seems out of character. Catching them early can spare a lot of anxiety later on.
Mid-to-Late Stage Escalation
As Alzheimers advances, the brains regulatory mechanisms wear down further, and seizure frequency often spikes. In late-stage disease, even a minor metabolic upsetlike a fevercan trigger a full-blown seizure.
Spotting the Signs
Focal Symptoms
Look for sudden jerking of a hand or foot, unexplained twitching, or a brief loss of awareness that lasts only a few seconds. Caregivers often describe it as the person spacing out in a way that feels different from typical confusion. Some specific reflexive movements, such as the fencing response seizure, can also be a clue that a seizure is occurring, especially in the context of neurological injury or disease.
Silent Seizures
These are the trickier ones. A silent seizure might appear as a short pause in conversation, a sudden blank look, or a brief episode where the person cant follow a simple question. Because theres no shaking, theyre easy to miss without an EEG.
Quick-Check Caregiver Checklist
| Observation | Possible Seizure Sign? |
|---|---|
| Staring blankly for 5-30 seconds | Silent seizure |
| Sudden involuntary twitch in one limb | Focal seizure |
| Brief episode of incomprehensible speech | Focal onset with speech involvement |
| Unexplained fall without loss of balance | Possible seizure-related fall |
How Are They Diagnosed?
Clinical Interview
First, your doctor will ask detailed questions about the episodeswhat happened, how long it lasted, and any triggers. A thorough medication review is also essential because some drugs can lower the seizure threshold.
EEG Testing
Electroencephalography is the gold standard for detecting abnormal brain waves. In Alzheimers, a routine EEG may miss silent seizures, so many specialists recommend a prolonged ambulatory EEG or even an overnight video-EEG to capture elusive activity.
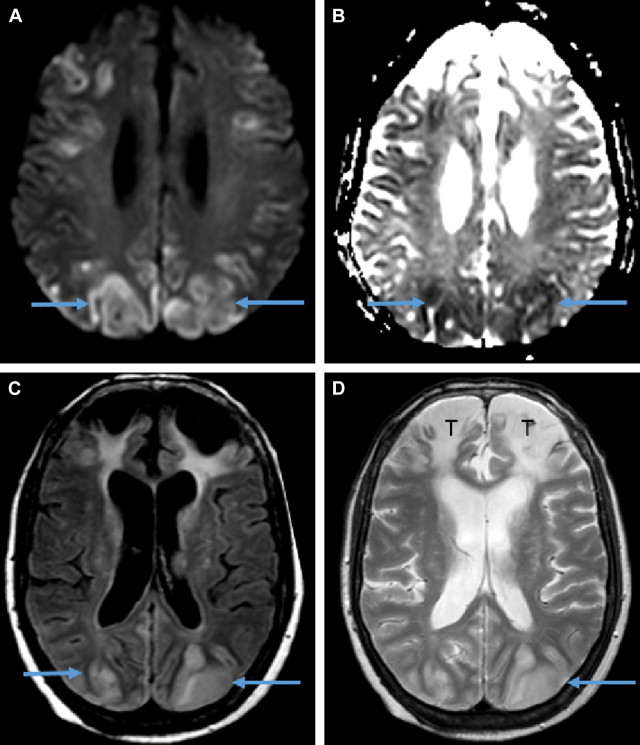
NeuroImaging
MRI or CT scans help rule out structural causes like tumors or large strokes. A recent review in Frontiers notes that combining EEG with advanced imaging improves diagnostic accuracy for dementia-related seizures.
Diagnostic Pathway (Summary)
- Initial clinical assessment & medication check.
- Standard EEGif negative but suspicion remains, proceed to prolonged EEG.
- MRI/CT to exclude other brain lesions.
- Integrate findings and discuss treatment options.
Treatment Options
First-Line Anti-Epileptic Drugs
Levetiracetam and lamotrigine are the most commonly prescribed AEDs for older adults because they have relatively mild cognitive side-effects. Studies show that low-dose levetiracetam can reduce seizure frequency without worsening memory in Alzheimers patients.
Drug-Interaction Tips
Many Alzheimers patients are already taking cholinesterase inhibitors (donepezil, rivastigmine) or memantine. Its crucial to monitor for interactionssome AEDs can increase liver enzymes or cause dizziness when combined with these medications. A collaborative approach with a neurologist and pharmacist is ideal.
Non-Pharmacologic Adjuncts
Improving sleep hygiene (consistent bedtime, reducing nighttime noise) can lower seizure risk. Stress-reduction techniques such as gentle yoga or guided breathing have modest evidence for stabilizing brain excitability. A small pilot study even explored the ketogenic diet in Alzheimers patients with seizures, showing promising seizure-control resultsbut its still experimental.
Medication Comparison Table
| AED | Typical Dose (mg) | Main Side-Effects | Interaction Notes |
|---|---|---|---|
| Levetiracetam | 250-500 BID | Fatigue, irritability | Generally safe with cholinesterase inhibitors |
| Lamotrigine | 25-100 BID | Rash, dizziness | Watch for additive CNS depression |
| Valproic Acid | 250-500 BID | Weight gain, thrombocytopenia | Higher risk of liver enzyme elevation |
Balancing Benefits & Risks
Cognitive Impact of Untreated Seizures
When seizures go unnoticed, they can accelerate cognitive decline. Research links uncontrolled seizures to a faster drop in MMSE scores and an increased risk of institutionalization. In short, treating seizures isnt just about preventing convulsionsits about preserving the quality of life.
Side-Effects of AEDs
Every medication carries tradeoffs. Some AEDs can cause dizziness, worsening balance, or even subtle memory lapses. Thats why starting at a low dose and titrating slowly, while closely monitoring cognitive function, is the safest route.
Decision-Making Box
Start treatment if: recurrent episodes, documented EEG spikes, or noticeable decline in daily functioning.
Consider watchful waiting if: isolated, brief events with no EEG confirmation and the patient is otherwise stable. Always discuss the pros and cons with your neurologist.
Prognosis & Life Expectancy
Effect on Disease Trajectory
Seizure occurrence is associated with a steeper decline in functional abilities. A large cohort study found that people with Alzheimers who had seizures were up to three times more likely to need full-time care within two years.
Statistics on Mortality
Seizures raise the risk of sudden unexpected death in epilepsy (SUDEP) and can contribute to cardiovascular complications. The American Epilepsy Society reports a 6-10-fold increase in mortality when seizures coexist with dementia.
Survival Overview (Narrative)
Imagine two parallel lines: one representing Alzheimers patients without seizures, the other with seizures. The line with seizures dips noticeably lower after the third year, reflecting a shorter median survivaloften a year or more less than their seizure-free peers.
Supporting Caregivers
Emotional Toll
Watching a loved one experience unpredictable episodes can feel like walking on a tightrope. Anxiety, guilt, and exhaustion are common. Acknowledging these feelings and seeking support is vitalnot a sign of weakness.
Practical Tips
- Keep a seizure log: date, time, description, possible trigger.
- Create an emergency plan: who to call, where to go, when to use emergency medication.
- Use medication reminder apps to avoid missed doses.
- Stay up-to-date on vaccination and infection controlfevers often precipitate seizures.
Resource Box
Helpful resources include the , local support groups, and online forums where caregivers share real-world strategies. Connecting with others can turn isolation into community.
Conclusion
Seizures are a real, often underrecognized part of the Alzheimers journey. By understanding why they happen, learning how to spot the subtle signs, and collaborating with healthcare providers on safe treatment options, you can protect both cognition and quality of life. If you suspect a seizure, dont waitschedule a professional evaluation, start a log, and lean on the support networks around you. You deserve clear answers and compassionate care, and so does your loved one.
FAQs
What are the most common signs of a seizure in someone with dementia?
Typical signs include brief staring spells, unexplained confusion, sudden jerky movements, or a sudden loss of awareness that lasts only a few seconds.
How is a seizure diagnosed when the person already has dementia?
Diagnosis usually starts with a detailed caregiver interview, followed by an EEG (often a prolonged or video‑EEG) and brain imaging (MRI or CT) to rule out other causes.
Which antiepileptic drugs are safest for older adults with dementia?
Levetiracetam, lamotrigine, brivaracetam, and low‑dose valproic acid are most often used because they have fewer drug‑drug interactions and are easier to titrate in the elderly.
Can lifestyle changes help reduce the risk of seizures in dementia?
Yes. Good sleep hygiene, controlling blood pressure, cholesterol, and diabetes, and reviewing all medications for seizure‑triggering side effects can lower seizure risk.
How do seizures affect life expectancy for people with dementia?
Studies show a 4‑6‑year reduction in median survival and a faster decline on cognitive tests (about 2‑3 MMSE points per year) compared with dementia patients who do not experience seizures.