Imagine watching a loved one struggle to lift a coffee mug or read a menu, and you feel helpless because you dont know if anything can actually help. The good news? Targeted Balint syndrome treatment can rebuild lost visualspatial skills and bring a bit of normalcy back to daily life.
In the next few minutes Ill walk you through the most effective therapies, share realworld success stories, and give you a clear checklist of what to ask your doctors. No jargon, just plainlanguage guidance you can act on right now.
Quick Facts
What is the classic Balint triad?
The syndrome is defined by three core symptoms, often called the Balint syndrome triad:
- Optic ataxia difficulty reaching for objects under visual guidance.
- Ocular (or oculomotor) apraxia trouble initiating or directing eye movements.
- Simultanagnosia inability to perceive more than one object at a time.
Which brain region is damaged?
Balints syndrome is associated with damage to the posterior parietaloccipital junction, especially the dorsal visual stream. This area integrates where information where objects are, how to reach them, and how to shift gaze.
What causes it?
Typical Balint syndrome cause includes:
- Ischemic stroke affecting posterior cortical territories.
- Traumatic brain injury.
- Hypoxicischemic events.
- Neurodegenerative disorders like posterior cortical atrophy.
How is it diagnosed?
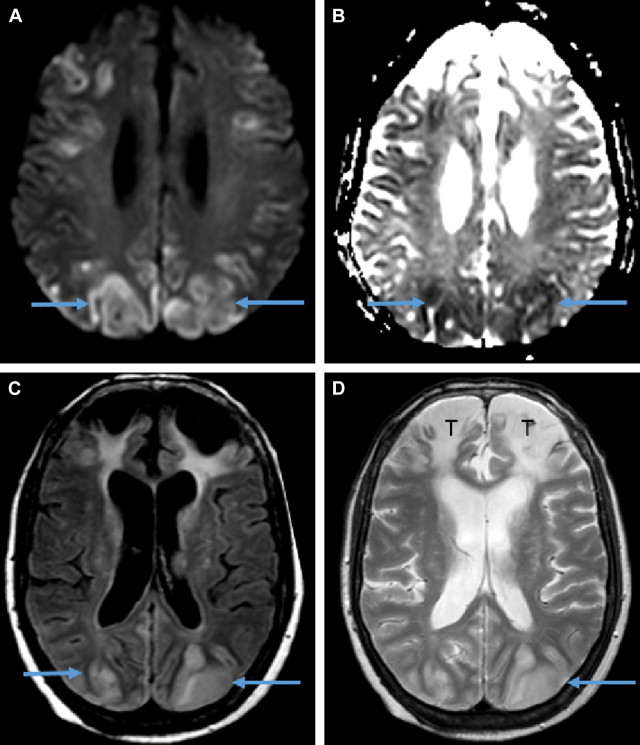
Diagnosis relies on a neuroophthalmologic exam, neuropsychological testing, and Balint syndrome radiology (MRI/CT). The imaging usually shows lesions in the parietaloccipital region.
| Imaging Modality | Typical Findings | Reference |
|---|---|---|
| MRI (T2/FLAIR) | Hyperintense lesions in posterior parietal cortex | |
| CT Scan | Areas of hypodensity in occipital lobes |
Why Treat?
Potential benefits
Effective Balint syndrome treatment can improve:
- Ability to perform everyday tasks reaching for a glass, buttoning a shirt, navigating a crowded room.
- Overall quality of life, as measured by patientreported outcome scales.
- Confidence and emotional wellbeing, because regaining independence feels empowering.
Risks and limits
Rehabilitation is intensive, and progress can be slow. Some patients experience frustration or fatigue, especially when visual tasks feel messy. In severe cases the ceiling for improvement may be modest, so its crucial to set realistic goals.
Setting expectations
Think of your rehab journey like learning a new language. You wont become fluent overnight, but consistent practice yields noticeable gains. A simple checklistshortterm goals (e.g., pick up a spoon) versus longterm goals (navigate a grocery aisle)helps keep expectations grounded.
Core Modalities
Occupational rehabilitation
Occupational therapists focus on functional tasks. They teach scanning strategies (e.g., look leftrightcenter before reaching) and break activities into bitesize steps. A typical homepractice list might include:
- Picking up coins from a tray.
- Tracing letters on a sheet.
- Reaching for a cup using a visual cue.
Visual (neurooptometric) therapy
Eyecare specialists use saccadic training, prism adaptation, and specialized software to retrain eyemovement control. One 2015 study in the Archives of Physical Medicine reported significant improvements in reaching accuracy after 12 weeks of VRT.
Neuropsychological protocols
Cognitive exercises target spatial awareness and working memory. Computerbased tasks such as find the odd shape among distractors can sharpen the dorsal stream. Recent PubMed case reports show that adding neuropsych training to occupational rehab boosts functional scores.
Adaptive strategies & assistive tech
When recovery plateaus, compensatory tools become essential. Lowtech options include:
- Largeprint utensils.
- Colorcoded kitchen items.
- Stickynote labels on doors.
Hightech alternatives range from eyetracking cursors to smartphone apps that provide auditory cues for navigation.
Pharmacological or surgical options?
Currently, no medication or surgery has proven efficacy for Balints core deficits. The consensus across and is that rehabilitation and adaptive strategies remain the mainstay.
Personalized Plan
Initial assessment checklist
Before you start, gather a multidisciplinary team:
- Neurologist to confirm lesion location.
- Neuroophthalmologist to assess optic ataxia severity.
- Occupational therapist to design functional drills.
- SVP therapist (visionperception) for visual scanning training.
- Neuropsychologist to address cognition and memory.
Setting SMART goals
Specific, Measurable, Achievable, Relevant, Timebound goals keep you motivated. Example:
Within four weeks, I will be able to pick up a passport from a table without assistance, using a visual cue at least 80% of the time.
Tracking progress
Use standardized tools like the Behavioral Inattention Test (BIT) or the VisualSpatial Accuracy Score. A simple spreadsheet can chart weekly scores, noting what exercises felt smooth versus messy.
When to adjust therapy
If improvement stalls after three months (<10% gain on BIT), consider adding visual therapy or switching to a highertech assistive device. A decisiontree graphic (not shown here) can guide those choices.
RealWorld Success Stories
Case 1 Fatembolism survivor
A 23yearold who suffered a fatembolism after orthopedic surgery showed marked progress after a combined occupational and neuropsych program. After six months, his Simultanagnosia score improved from severe to mild, and he could navigate a supermarket aisle independently ().
Case 2 Young visualtherapy champion
At 19, a college student with optic ataxia underwent intensive VRT for 12 weeks. His reaching accuracy rose from 40% to 85%, and he reported feeling like my brain finally got the memo about where my hands should go ().
Lessons learned
Across both stories, key factors emerged: consistent home practice, supportive family members, and early involvement of a multidisciplinary team. Insurance hurdles were common, but patients who appealed denials with detailed therapist notes often secured coverage if you need help with coverage for medications or therapies, resources such as Exondys 51 insurance programs can offer a model for navigating approvals and appeals.
BottomLine Takeaways
Balint syndrome treatment isnt a quick fix, but its far from hopeless. By blending occupational rehab, visualtherapy drills, neuropsych protocols, and smart adaptive tools, most patients see meaningful improvements in daily functioning. Your next step? Schedule a comprehensive assessment with a neuroophthalmologist and an occupational therapist, grab the free Balint Rehab Planner PDF (linked below), and join a supportive community of people walking the same road.
Remember, progress may feel like peeling an onionlayer by layer, sometimes with a sting, but every layer brings you closer to the core of independence. If you have questions or want to share your own journey, feel free to comment below. Were all in this together.
FAQs
What are the first steps after a Balint syndrome diagnosis?
Begin with a comprehensive assessment by a neurologist, neuro‑ophthalmologist, occupational therapist, and neuropsychologist to map deficits and plan a personalized rehabilitation program.
How does occupational therapy help with optic ataxia?
Occupational therapists teach scanning strategies, break tasks into small steps, and use repetitive functional drills (e.g., picking up objects) to re‑train hand‑eye coordination.
Can visual (neuro‑optometric) therapy improve eye‑movement control?
Yes. Saccadic training, prism adaptation, and computer‑based eye‑movement exercises have shown significant gains in reaching accuracy and gaze stability after several weeks of consistent practice.
Are there any medications that treat the core symptoms of Balint syndrome?
Currently, no drugs or surgical procedures directly address optic ataxia, oculomotor apraxia, or simultanagnosia. Rehabilitation and adaptive strategies remain the main evidence‑based approaches.
What adaptive tools can assist daily living when progress slows?
Low‑tech options like large‑print utensils, color‑coded kitchen items, and sticky‑note labels, as well as high‑tech solutions such as eye‑tracking cursors or smartphone navigation apps, help maintain independence.