Why does this matter? Imagine youve felt a strange pinsandneedles sensation in your toes for weeks. Youre scared it might be ALS, but you also know that peripheral neuropathy is far more common. Getting clarity means you can talk to your neurologist with confidence, avoid unnecessary anxiety, and get the most appropriate carewhether thats a nerveconduction study, a medication for diabetesrelated neuropathy, or a referral to an ALS specialty clinic.
Neuropathy vs ALS
First things first: lets untangle the basics. Neuropathy is a blanket term for damage to the peripheral nervesthose that run from your spinal cord out to your feet, hands, and everything in between. It can be caused by diabetes, vitamin deficiencies, infections, or even certain medications. The hallmark symptoms are numbness, tingling, burning, and sometimes weakness, but the nerves that control muscle movement are usually spared.
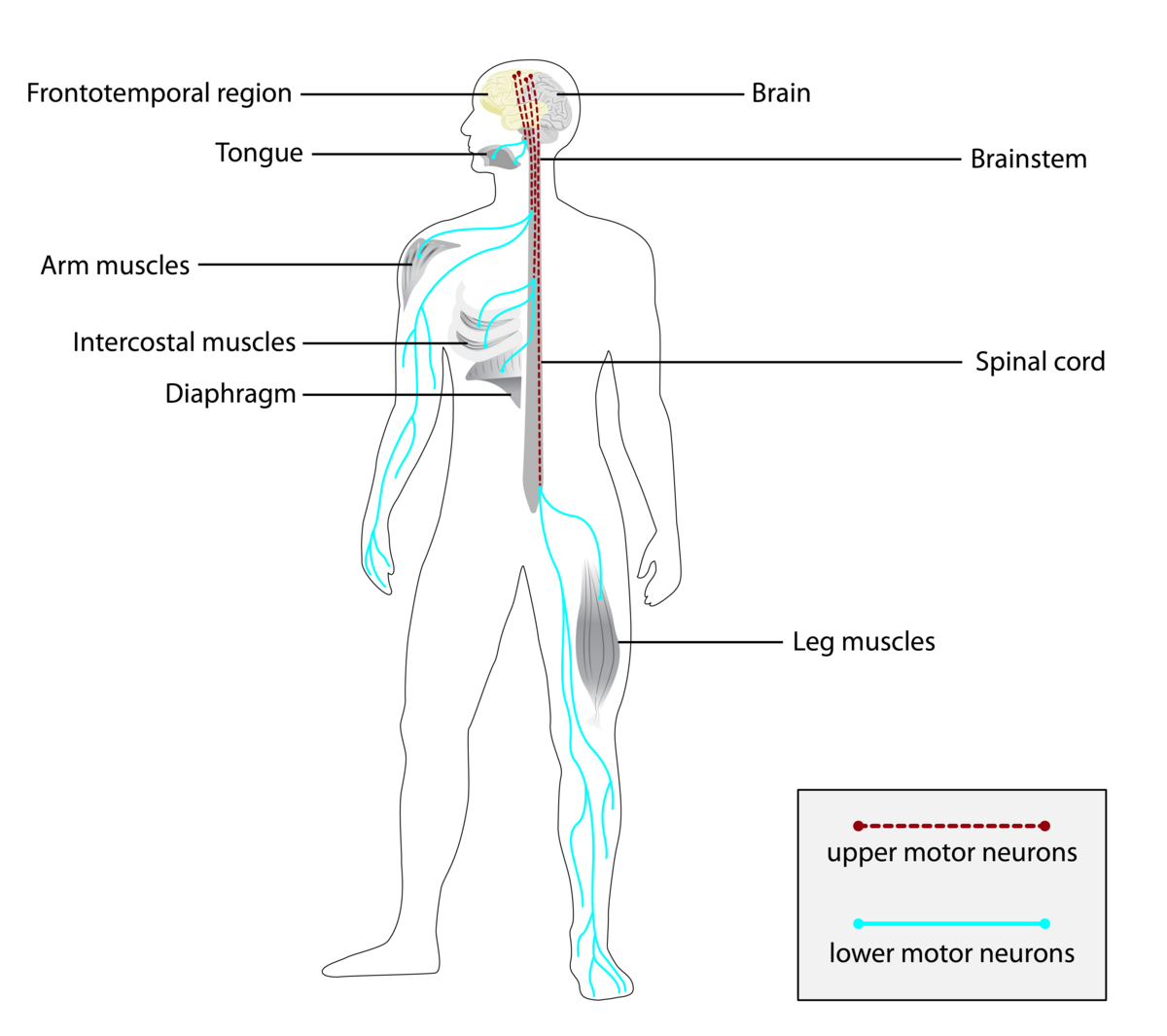
ALS (amyotrophic lateral sclerosis), on the other hand, is a progressive motorneuron disease. It attacks the nerve cells that tell your muscles to move, leading to muscle weakness, cramping, and eventually paralysis. Sensory nerves are generally untouched, which is why most people think ALS doesnt cause numbness. Yet, a small slice of patients do report sensory changes, and thats where the confusion begins.
| Feature | Typical in Neuropathy | Typical in ALS | Possible in Both |
|---|---|---|---|
| Numbness / Tingling | Common (hands, feet) | Rare (1020% cases) | Yes (especially early) |
| Muscle Weakness | Secondary to nerve loss | Primary, progressive | Yes |
| Muscle Atrophy | Gradual, often distal | Rapid, widespread | Yes |
| Reflex Changes | Reduced or absent | Hyperreflexia (spasticity) | Variable |
When you look at that table, the line that blurs most often is the Numbness/Tingling row. Thats why the next section is worth a closer look.
ALS Sensory Neuropathy
So, does ALS really cause a peripheralnervetype neuropathy? found that about onefifth of their ALS cohort reported mild sensory symptoms, mostly in the feet. The researchers used EMG and nerveconduction studies to confirm that these sensations werent from a separate diabetic neuropathythey were subtle changes in largefiber pathways that happen alongside motorneuron loss.
Whats happening inside the body? ALS primarily destroys upper and lower motor neurons, but the disease can also trigger inflammation that affects neighboring sensory fibers. Think of it like a city where the power grid (motor neurons) gets knocked out, but the streetlights (sensory fibers) flicker a bit before going dark. Most patients notice the flicker as a mild tingling, not a fullblown loss of feeling.
Heres a quick snapshot from five realworld cases (anonymized for privacy):
- Case1: A 58yearold teacher felt walking on cotton in her feet for six months before developing hand weakness. EMG showed classic ALS patterns; nerveconduction studies were normal except for a slight slowing of sensory velocity.
- Case2: A 45yearold marathon runner reported occasional electric shocks in his calves. After ruling out vitamin B12 deficiency, his neurologist diagnosed earlystage ALS.
- Case3: A 62yearold retired chef complained of burning sensations in her fingers; months later, she experienced pronounced tongue fasciculationsan unmistakable ALS sign.
- Case4: A 39yearold office worker noticed tingling in both palms, which he first blamed on keyboard strain. Within a year, gait changes forced a specialist referral.
- Case5: A 71yearold farmer experienced numbness in his big toes. The subsequent rapid progression of leg weakness and hyperreflexia pointed to ALS.
These stories illustrate that while sensory symptoms can appear, they rarely dominate the clinical picture. Still, theyre a critical clue, especially when they accompany early muscle weakness. If you or a loved one are wondering about supportive services or how insurance covers treatments, resources on Exondys 51 insurance and assistance programs can be useful models for navigating coverage questions for rare neurological therapies.
Common Questions
Lets dive into the burning questions you (or someone you love) might be Googling right now.
How can you tell you dont have ALS?
If you havent noticed progressive, asymmetrical muscle weakness, especially in the hands or speech muscles, the odds are low. Redflag signs that usually dont appear in ALS include persistent pain (more typical of neuropathy) and a strictly sensory loss without motor involvement.
Whats the key difference between peripheral neuropathy and ALS?
Peripheral neuropathy primarily knocks out sensation firstthink pinsandneedles that spread from toes upward. ALS flips the script: you feel a sudden loss of strength, often in the thumb, hand grip, or speech, before any tingling shows up.
Does ALS cause numbness in the feet?
Rarely, but yes. Around 1020% of ALS patients report mild foot numbness. If its the only symptom for months, a separate neuropathy is more plausible.
Why might ALS patients feel tingling?
Inflammation around dying motor neurons can irritate nearby sensory fibers, creating brief tingling episodes. Its usually fleeting and less intense than the chronic burning seen in diabetic neuropathy.
Are early ALS signs different for women?
Women often notice subtle hand weakness or clumsiness first, rather than the dramatic leg weakness more common in men. Some research () suggests women may present slightly later, making sensory clues (like tingling) even more valuable for early detection.
Is peripheral neuropathy a symptom of ALS?
Its not a defining symptom, but it can coexist. Think of it as an accessory player: not the main storyline, but it can appear in a minority of cases.
What causes ALS?
Most cases are sporadic, likely a mix of genetics, environmental exposures, and cellular stress. About 510% are hereditary, linked to mutations in genes like SOD1 or C9orf72. Lifestyle factors (smoking, intense physical activity) have been explored, but the exact trigger remains a puzzle.
How is hand weakness tested in ALS?
Neurologists often use a gripstrength dynamometer or the ALS handwrist test, where you try to make a fist and then extend the fingers against resistance. A drop in strength over weeks is a red flag.
Diagnostic Pathway
Getting the right diagnosis is a bit like solving a mystery: you gather clues, rule out suspects, and then confirm the culprit with the gold standard test.
- Step1 Clinical Exam: Your doctor checks reflexes, muscle tone, and sensation. Hyperreflexia (overactive reflexes) leans toward ALS; diminished reflexes point to neuropathy.
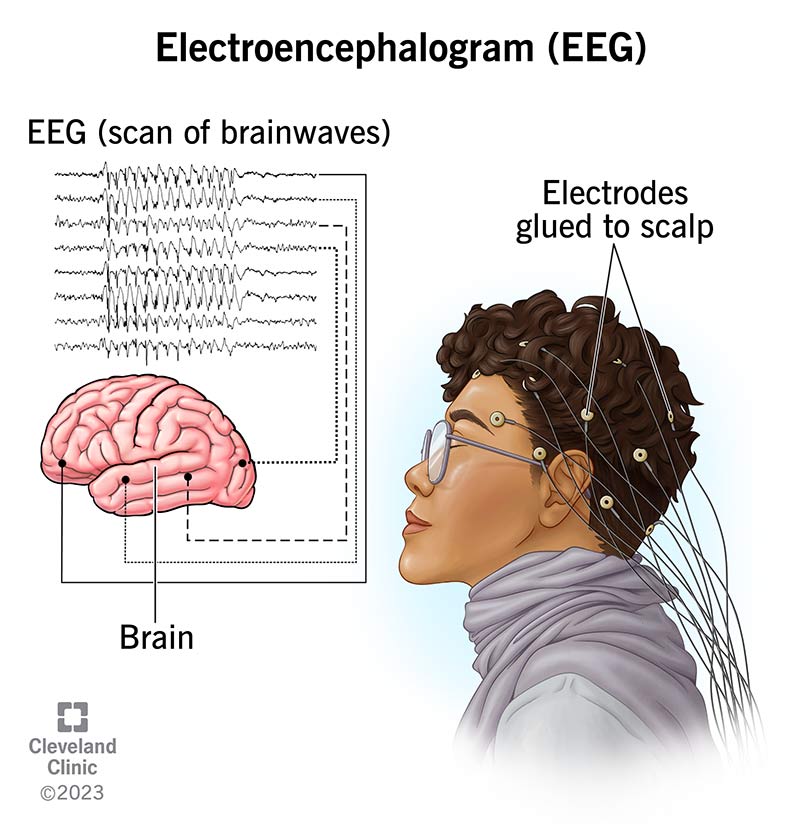
- Step2 Electromyography (EMG) & NerveConduction Studies (NCS): EMG reveals denervated muscle fibers typical of ALS, while NCS measures how fast sensory nerves conductabnormal speeds suggest peripheral neuropathy.
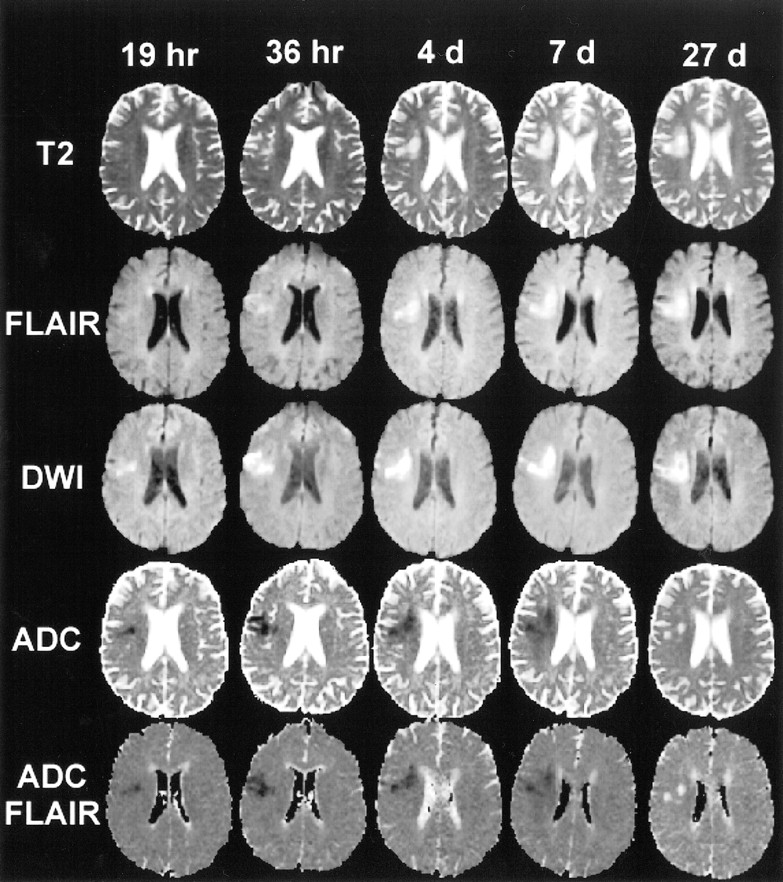
- Step3 Imaging & Biomarkers: MRI rules out spinal cord lesions, and blood tests for neurofilament light chain can support an ALS diagnosis ( in ALS patients).
- Step4 Specialized Clinics: Multidisciplinary ALS centers provide comprehensive evaluation and can confirm subtle sensory involvement.
Below is a simple flowchart you can keep on your fridge (or just picture it in your head):
| Start | Check for Motor Weakness | EMG/NCS | Result |
|---|---|---|---|
| Patient reports tingling | Yes Proceed to EMG | Motoronly changes ALS likely Sensory changes only Neuropathy likely | Refer to appropriate specialist |
Management Options
Even though ALS is a challenging diagnosis, there are treatments that can slow progression and improve quality of life. And if youre dealing with a plainvanilla peripheral neuropathy, a whole different toolbox opens up.
ALSFocused Therapies
- Riluzole: The first FDAapproved drug; modestly extends survival by a few months.
- Edaravone: An antioxidant that may slow functional decline in a subset of patients.
- Multidisciplinary Care: Physical therapy, speech therapy, and nutritionists form a safety net that can keep independence longer.
NeuropathyFocused Treatments
- Medication: Gabapentin, pregabalin, or duloxetine for painful tingling.
- Address Root Causes: Tight bloodsugar control for diabetic neuropathy, vitamin B12 supplementation if deficient.
- Physical Therapy: Strengthens unaffected muscles and reduces fall risk.
Overlap Relief
When ALS patients also feel numbness, a joint approach works best. Occupational therapists can customize hand splints that protect fragile muscles while alleviating tingling. Foot orthotics can cushion the soles for those with foot numbness, preventing skin breakdown.
Lifestyle Checklist
- Stay activegentle walks or swimming keep muscles supple.
- Prioritize a balanced diet rich in antioxidants (berries, leafy greens).
- Mindbody practices (yoga, meditation) help manage anxiety that often accompanies chronic illness.
- Keep a symptom journal; patterns help your doctor finetune treatment.
RealWorld Stories
Stories stick in our memory better than bullet points. Here are two short vignettes that bring the data to life.
I thought my tingling meant I had ALS
Mark, a 52yearold accountant, started feeling pinsandneedles in his right foot during his daily commute. He Googled ALS numbness and frightened himself. After a thorough exam, his neurologist found normal sensory NCS and diagnosed earlystage peripheral neuropathy from a mild vitamin D deficiency. Marks symptoms cleared with supplementation and a new ergonomic shoe insert. His story reminds us: a single symptom rarely tells the whole tale.
Clinicians Dilemma
Dr. Patel, a boardcertified neurologist, describes a patient who presented with subtle foot tingling and a barely noticeable hand grip decline. EMG showed motorneuron loss, while NCS was normal. She explained that the tingling threw us off at first, but the electrophysiology sealed the ALS diagnosis. Dr. Patel now always asks patients with ALS about any sensory changes, ensuring she doesnt miss that minority of cases where the two overlap.
Quick Answers
- Does ALS cause numbness in feet? Only in a small minority (1020%); most foot numbness is due to other neuropathies.
- How to differentiate ALS from peripheral neuropathy? Look for progressive motor weakness, hyperreflexia, and EMG evidence of motorneuron loss; neuropathy shows sensory loss first and reduced reflexes.
- What is the ALS hand weakness test? A gripstrength dynamometer measurement combined with resisted finger extension; decreasing scores over weeks suggest ALS.
These bitesize answers are perfect for a quick scroll, but the deeper dive above gives you context and confidence.
Final Thoughts
Understanding the blurry line between neuropathy and ALS can feel like navigating a foggy road, but you dont have to travel it alone. Remember: ALS is primarily a motorneuron disease; sensory tingling is an occasional sideguest, not the main act. If you notice any new numbness, tingling, or unexplained weakness, schedule an appointment with a neurologist who can run EMG and NCS teststhose are the Sherlock Holmes tools that separate ALS from a regular neuropathy.
Take heart, though. Whether youre dealing with ALS, a simple peripheral neuropathy, or the uncertainty between the two, there are specialists, support groups, and evidencebased treatments ready to help. Share your story in the commentsyour experience might be the clue someone else needs. And if you have questions, dont hesitate to ask; were all in this learning journey together.
FAQs
Can ALS cause numbness or tingling in the feet?
Yes, but it’s uncommon. Approximately 10‑20 % of ALS patients report mild foot numbness or tingling, usually alongside early motor symptoms.
What are the main clinical differences between peripheral neuropathy and ALS?
Peripheral neuropathy starts with sensory loss (numbness, burning) and reduced reflexes, while ALS begins with progressive muscle weakness, hyperreflexia, and motor‑neuron signs.
How do doctors distinguish ALS from neuropathy during testing?
Electromyography (EMG) shows denervation patterns in ALS, whereas nerve‑conduction studies reveal slowed sensory velocities in peripheral neuropathy. Reflex patterns also help differentiate.
Is sensory loss ever a red‑flag symptom for early ALS?
It can be a clue, especially when mild tingling appears with subtle hand or tongue weakness. However, isolated sensory loss without motor involvement is more typical of neuropathy.
What treatment options exist for patients who have both ALS and peripheral‑type sensory symptoms?
ALS‑focused therapies (riluzole, edaravone, multidisciplinary care) are combined with neuropathy‑targeted measures such as gabapentin for pain, vitamin supplementation, and orthotic support for foot comfort.