Why does this matter to you or a loved one? Because every ticking minute can determine whether lifesaving treatments like clotbusting drugs or mechanical thrombectomy are still an option. Knowing both the scantime and the clinical timeline helps you ask the right questions in the emergency room and understand the decisions your medical team makes.
Two Faces of Duration
What stroke MRI duration really means
In everyday conversation the phrase can be confusing. Doctors usually refer to:
- Acquisition time the period the MRI machine is actually scanning your brain. This is the 3090minute number youll see on patientinformation sheets.
- Onsettoimaging interval the elapsed time from when stroke symptoms first appear to the moment the MRI starts. This clock is what determines eligibility for treatments like intravenous tPA (up to 4.5hours) and thrombectomy (up to 624hours in selected cases).
Key data point
According to a 2023 study published in , the median onsettoMRI time across 1,200 acute stroke patients was 114minutes (interquartile range 89138minutes). This figure gives you a realistic sense of how fast top hospitals can mobilize.
Typical scantime for a stroke MRI
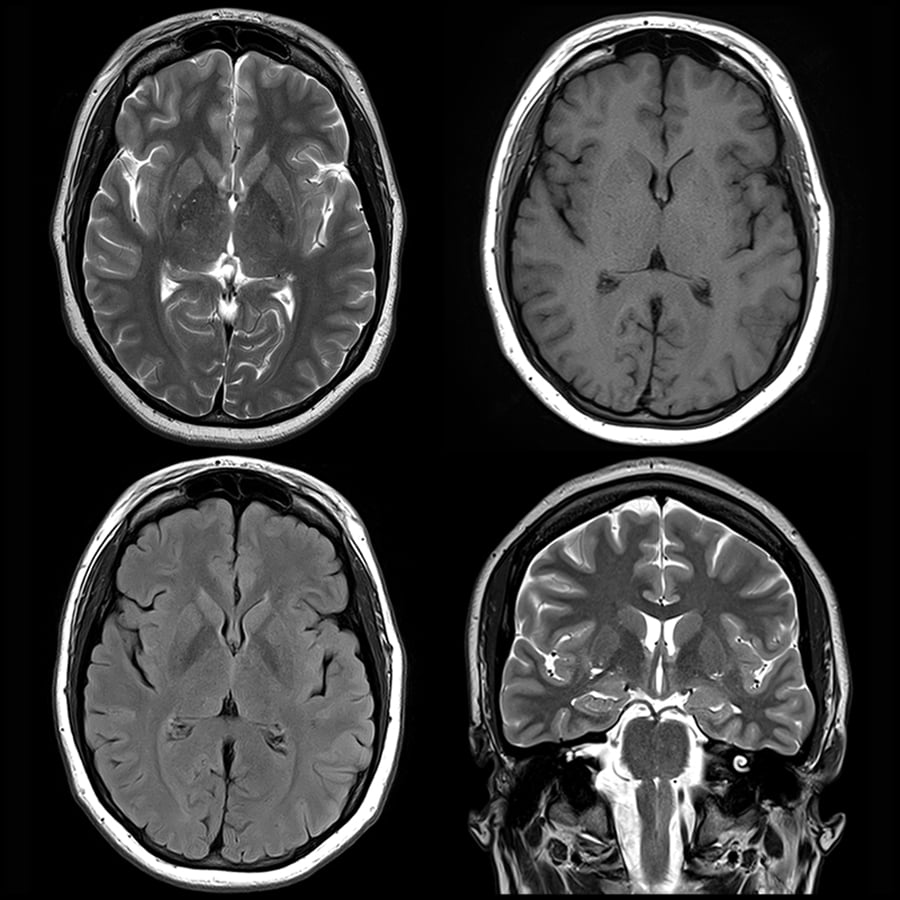
When you step into the magnet, a series of sequences run one after the other:
- Diffusionweighted imaging (DWI) about 5minutes. This is the hero sequence that spots a new infarct within minutes of symptom onset.
- T1weighted and T2weighted images 1015minutes combined, painting a detailed picture of brain anatomy.
- FLAIR and ADC maps another 510minutes, helping differentiate acute from subacute changes.
- Optional contrastenhanced MRA adds 510minutes if the physician wants to see the blood vessels.
All together, a comprehensive acute stroke protocol usually wraps up in 3090minutes. Most patients hear the youll be done in about an hour line, which is a reasonable ballpark.
Patient tip
Bring earplugs or headphones, practice calm breathing, and let the technologist know if youre claustrophobic. The scanner is noisy, but the whole thing finishes before you can finish a coffee break.
Why the onsettoimaging window matters
Think of stroke treatment like catching a train that only departs every few minutes. If you miss the first train (the early imaging), you might still catch a later one (thrombectomy), but youll have fewer seats (brain tissue) left.
- IVtPA must start within 4.5hours of symptom onset, and the sooner the better each 15minute delay reduces the chance of a good outcome by about 5%.
- Mechanical thrombectomy can be performed up to 24hours in selected patients, but only if advanced imaging (often MRI perfusion) shows salvageable tissue.
In short, a short stroke MRI duration (both acquisition and onsettoimaging) opens the door to more therapeutic options.
Stroke Visibility Timeline
When MRI first sees a stroke
Diffusionweighted imaging is incredibly sensitive. Within minutes of an ischemic event, water molecules in the affected brain area become restricted, lighting up bright on DWI. Studies show DWI detects >80% of acute strokes within the first hour.
How long the lesion stays on MRI
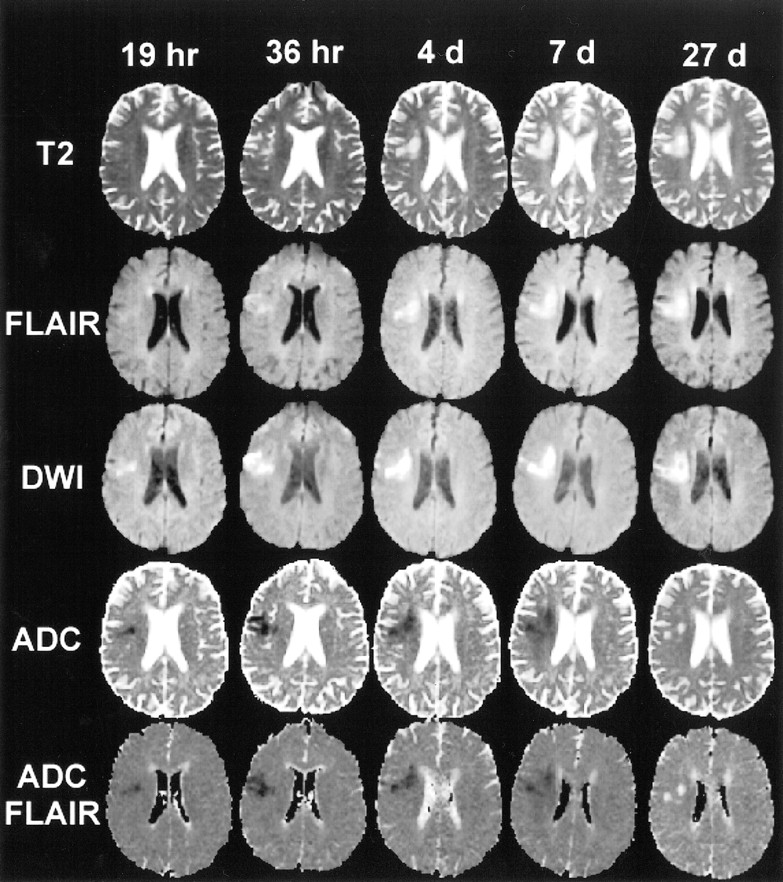
After the acute phase, the appearance evolves:
- First 324hours T2 and FLAIR signals start to rise, helping radiologists confirm the age of the infarct.
- Days to weeks the affected tissue becomes a darker, chronic cavity on T1 and T2, essentially a scar that can linger for months or years.
So, a stroke can be visible on MRI for the rest of a persons life, but the imaging characteristics change over time.
CT vs. MRI: When each shows the stroke
Noncontrast CT is faster usually 510minutes but its sensitivity in the first 6hours can be as low as 3040%. MRI outshines CT in the hyperacute window, especially for small, posteriorcirculation or lacunar strokes.
Can MRI predict a stroke before it happens?
Not exactly, but MRI can spot silent infarcts or extensive whitematter hyperintensities that signal a higher future risk. A 2023 review in Radiology highlights that patients with many silent lesions have a 23fold increased chance of a symptomatic stroke within the next five years.
MRI or CT? Making the Right Choice
When MRI is the first pick
If youre within 12hours of symptom onset, have no contraindications (like certain metal implants), and your hospital has a 24/7 MRI, doctors often choose MRI because it gives a clearer map of:
- Exact size and location of the infarct (DWI).
- Presence of penumbra tissue at risk but still salvageable (perfusion MRI).
- Vessel status via MR angiography (MRA).
When CT still wins
CT is the goto when speed is paramount, the patient is unstable, or MRI is unavailable. Its also essential to rule out intracerebral hemorrhage, which appears bright on CT right away.
MRI with or without contrast
Contrast agents (gadolinium) boost vessel visibility and help detect bloodbrain barrier breakdown. However, they add a few extra minutes and a small risk of allergic reaction or nephrogenic systemic fibrosis in patients with severe kidney disease. Current AHA/ASA guidelines (2022) suggest using contrast only when vessel imaging or tumorlike lesions need clarification.
Impact on treatment timelines
Adding MRI can increase the doortoneedle time by roughly 515minutes, but the richer information often leads to more tailored therapy. For example, a patient with a large penumbra on perfusion MRI might qualify for thrombectomy even after the conventional 6hour window.
Patientexperience checklist
- Confirm youre not pregnant.
- Remove all metal (including jewelry).
- Tell the technologist about any implants.
- Ask about ear protection and the length of the scan.
- Know whether contrast will be used and discuss any kidney concerns.
RealWorld Stories
Case A Fast MRI saves tissue
John, 62, felt sudden weakness in his right arm while gardening. EMS arrived in 7minutes, and the nearest stroke center logged his symptoms at 08:15. By 09:28 (just over an hour later) he was on the MRI table. DWI showed a small leftmiddleterritory infarct. Because the MRI was done within the 114minute average, the team gave IVtPA at 09:45, well before the 4.5hour cutoff. John reclaimed full use of his arm within days.
Case B Delayed MRI misses the window
Maria, 48, woke with slurred speech and visual loss. She waited at home for 2hours before calling emergency services. By the time she reached the hospital, the MRI started at 11:45, more than 5hours after onset. The scan confirmed a large ischemic core, and the team couldnt administer tPA. Later, she underwent thrombectomy, but some permanent visual field loss remained. This story highlights how every minute counts.
What to ask your ER team
Can we get an MRI as soon as possible?
Is a contrastenhanced study needed?
How long will the scan take, and whats the expected doortotreatment time?
Bottom Line Balancing Speed, Accuracy, and Comfort
When you hear stroke MRI duration, think of two clocks ticking side by side: the scanners 3090minute runtime, and the clinical onsettoimaging window that usually averages around 1hours in top centers. Both matter.
- Speed matters. The faster youre imaged, the more therapeutic options stay on the table.
- Accuracy matters. MRI gives a detailed view of the infarcts size, age, and surrounding tissue.
- Patient comfort matters. Knowing what to expect (noise, length, contrast) reduces anxiety and helps you stay still for clearer images.
In the emergency setting, dont be shy about asking whether MRI is feasible and how long it will take. Your questions can shave precious minutes off the clock.
Conclusion
In a nutshell, a stroke MRI takes 3090minutes to perform, but the pivotal stroke MRI duration for treatment decisions is roughly 1.5hours from symptom onset to imaging. Getting that scan done quickly can be the difference between a full recovery and lingering deficits. If you or someone you love experiences stroke symptoms, ask the emergency team about the expected MRI timeline and whether CT might be faster in that specific moment. Stay informed, stay prepared, and remember that timely imaging truly saves lives.
Feel free to download our printable Stroke Imaging Timeline checklist below, and let us know in the commentswhat questions would you ask your doctor in an emergency? Your experience could help someone else navigate this critical moment.
For caregivers managing complex neurologic diagnoses, resources on atypical Rett syndrome may offer useful guidance about care coordination and urgent evaluation when sudden neurologic changes occur.
FAQs
What is the typical acquisition time for a stroke MRI?
The scan usually takes between 30 and 90 minutes, depending on the protocol and whether contrast imaging is added.
How does “onset‑to‑imaging” differ from scan time?
Onset‑to‑imaging measures the minutes from symptom start until the MRI begins, a key factor for treatment eligibility, while scan time is the actual duration the machine runs.
Can a CT scan replace MRI in the hyper‑acute stroke setting?
CT is faster and excellent for ruling out hemorrhage, but MRI, especially diffusion‑weighted imaging, detects ischemic strokes earlier and more accurately.
Is contrast always required for a stroke MRI?
Contrast (gadolinium) is optional; it helps visualize vessels and blood‑brain barrier breakdown but adds a few minutes and is avoided in severe kidney disease.
What can I do to prepare for a stroke MRI?
Remove all metal, inform the technologist about implants, bring ear protection, and let them know if you’re claustrophobic; this helps keep the exam smooth and quick.