Lets cut to the chase: a colitis biomarker test can tell you whether the inflammation in your gut is heating up, cooling down, or staying steadyoften without the need for an uncomfortable colonoscopy. Below you'll discover which blood and stool markers are most reliable, how to interpret the numbers, and what steps to take next so you can feel confident talking with your doctor.
Why Biomarkers Matter
What Exactly Is a Biomarker?
Think of a biomarker as a tiny messenger that travels in your blood or stool, whispering clues about what's happening inside your intestines. It's not a fancy term for test result; it's the body's own signal that doctors can read to gauge inflammation, disease activity, and even how well a medication is working.
How Biomarkers Help Your Doctor
Because they're noninvasive, biomarkers let gastroenterologists monitor you more often than they could with colonoscopies alone. They can spot a flare before you notice severe symptoms, help decide whether to updose a biologic, and even differentiate Crohn's disease blood test markers from ulcerative colitis.
Key Takeaway
Biomarkers are the shortcut to what's really going on without the hassle of an endoscopic procedure.
Commonly Used Biomarkers
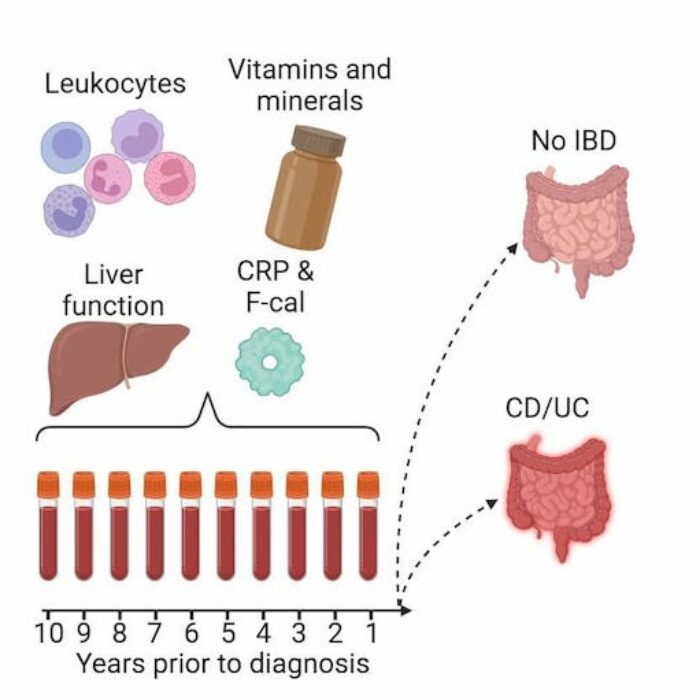
- C-reactive protein (CRP): A quick blood test that rises when there's systemic inflammation.
- Fecal calprotectin (FCP): A stool test considered the gold standard for detecting gut inflammation.
Supporting Data
According to the research, fecal calprotectin has higher specificity for inflammatory bowel disease (IBD) than CRP alone.
Emerging or Specialty Markers
- ASCA (Anti-Saccharomyces cerevisiae antibodies) & pANCA: Often ordered as an antibody blood test for Crohn's disease to help differentiate it from ulcerative colitis.
- Cytokine panels & genetic tests: Still mostly research tools, but they show promise for personalized treatment plans.
Pros & Cons Table
| Marker | Sensitivity | Specificity | Cost (USD) | Turnaround |
|---|---|---|---|---|
| CRP (blood) | 7080% | 6070% | ~$20 | Same day |
| Fecal Calprotectin | 8595% | 8090% | ~$70 | 23 days |
| ASCA/pANCA (antibody) | 5565% | 7080% | ~$100 | 1 week |
Types of Tests
Blood Tests You'll Likely Encounter
- Blood test for ulcerative colitis: Checks CRP, ESR, CBC, and sometimes antibody panels.
- Crohn's disease blood test markers: Looks at ASCA, pANCA, and CRP to help differentiate Crohn's from UC.
- Antibody blood test for Crohn's disease: Specifically measures ASCA IgA/IgG.
- IBD blood test results: Includes a full pictureCBC for anemia, electrolytes, and inflammation markers.
Stool Tests You May Need
- IBD blood test calprotectin: Actually a stool test; measures fecal calprotectin levels.
- Stool test for Crohn's disease / ulcerative colitis: Often combines calprotectin with lactoferrin and occult blood.
- Comprehensive stool panel: May add microbiome analysis for a more holistic view.
Comparison Table
| Test | Sample | What It Detects | Typical Use | Key Related Keyword |
|---|---|---|---|---|
| Blood test for ulcerative colitis | Blood | CRP, ESR, CBC, antibodies | Baseline & flare check | blood test for ulcerative colitis |
| Crohn's disease blood test markers | Blood | ASCA, pANCA, CRP | Differentiating CD vs UC | crohn's disease blood test markers |
| Fecal calprotectin | Stool | Gut inflammation | Monitor activity, rule out IBS | ibd blood test calprotectin |
| Stool test for ulcerative colitis | Stool | Calprotectin, occult blood | Assess flare severity | stool test for ulcerative colitis |
How to Prepare for Each Test
Blood tests: Most require a simple fast of 812 hours if a lipid panel is included, but CRP and CBC are fine no-fasting. Bring a list of current medssome anti-inflammatories can spike CRP.
Stool collection: Use the kit your doctor or lab provides. Grab a small sample (about the size of a grape), avoid mixing with urine, and seal it tightly. Store it in the fridge if you can't drop it off the same day.
Step-by-Step Stool Collection (quick cheat sheet)
- Wash hands thoroughly.
- Open the collection container.
- Use the provided spatula to transfer stool onto the collection paper.
- Place the paper into the container, seal, and label.
- Put the container in the fridge (4C) until you drop it off.
Interpreting Results What Do the Numbers Mean?
Every laboratory has its own reference ranges, but here's a quick rule of thumb:
- CRP: <5mg/L is generally normal; 510mg/L may indicate mild inflammation; >10mg/L often points to an active flare.
- Fecal calprotectin: <50g/g is usually considered normal; 50200g/g may suggest mild disease; >200g/g is strongly associated with active IBD.
- ASCA/pANCA: Positive ASCA leans toward Crohn's; positive pANCA leans toward ulcerative colitis, but many patients test negative for both.
Case Study: Emma's Flare
Emma, 32, was feeling off but not sick enough to see a gastroenterologist. Her doctor ordered a fecal calprotectin test. The result came back at 280g/gwell above the 200g/g threshold. Within a week, her medication was adjusted, and her symptoms improved dramatically. Emma's story illustrates how a simple stool test can catch a flare before it wrecks your day.
Benefits & Risks
Why You'll Love These Tests
- Early detection: Spot a flare before it escalates to hospitalization.
- Personalized treatment: Adjust meds based on objective data, not just symptoms.
- Less invasive: Reduce the frequency of colonoscopies, which are costly and uncomfortable.
Expert Insight
Dr. Maya Singh, a board-certified gastroenterologist, says, "Biomarkers give us a window into the gut without the need for a camera. They're especially valuable for patients who can't tolerate frequent endoscopies."
Potential Drawbacks
- False positives/negatives: NSAIDs, infections, or even a recent diet change can skew CRP or calprotectin levels.
- Cost & coverage: While many insurers cover CRP, fecal calprotectin may require prior authorization.
- Interpretation challenges: Not all elevations mean a severe flare; clinical context matters.
Balanced Comparison Chart
| Aspect | Benefit | Risk / Limitation |
|---|---|---|
| Early detection | Can prevent hospital visits | May miss very mild flares |
| Noninvasive | No sedation needed | Stool collection can be awkward |
| Cost | Generally cheaper than colonoscopy | Insurance coverage varies |
When to Order a Test
Clinical Situations That Prompt Testing
- New or worsening symptoms (diarrhea, abdominal pain, blood in stool).
- Routine monitoring every 612 months, as recommended by the guidelines.
- Before changing or initiating biologic therapy.
- When you're tapering steroids and need objective proof of remission.
Talking to Your Doctor
Keep a short list of questions ready:
- Which biomarker best reflects my disease activity?
- How often should I repeat the test?
- What could affect the results (meds, diet, infection)?
- Will my insurance cover this test?
Decision-Tree Graphic (text version)
Start: New symptoms or routine check? Yes: Order CRP and fecal calprotectin. Result high? Discuss medication adjustment. Result low? Continue current plan, monitor.
Practical Action Plan
Step-by-Step Checklist for You
- Schedule a conversation with your gastroenterologist about which markers suit your situation.
- Arrange the blood draw (fasting if required) and request a stool kit.
- Log daily symptoms, medication doses, and any recent illnesses or NSAID use.
- Submit the stool sample within 24 hours of collection.
- Review results with your doctor, focusing on trends rather than isolated numbers.
- Adjust treatment as advised, then repeat testing according to the agreed schedule.
Downloadable Tracker
Use our printable Colitis Test Tracker (Excel) to keep everything in one placetest dates, results, symptom scores, and medication changes.
Reliable Resources for Further Reading
- .
- .
- .
Conclusion
A colitis biomarker test is a fast, noninvasive way to gauge inflammation, guide treatment, and catch flares before they disrupt your life. By understanding the main blood and stool markersCRP, fecal calprotectin, and disease-specific antibodiesyou can have informed conversations with your doctor and take proactive steps in managing IBD. Remember, biomarkers are tools, not replacements for endoscopic evaluation, so keep the dialogue open, stay on top of testing schedules, and use the resources listed to stay empowered. If you've tried these tests before, share your experience in the comments; let's learn from each other and keep the conversation going.
FAQs
What is the difference between a blood test and a stool test for colitis?
Blood tests (like CRP) measure systemic inflammation, while stool tests (such as fecal calprotectin) directly assess inflammation within the gut. Stool tests are generally more specific for IBD activity.
How should I prepare for a colitis biomarker test?
Blood draws usually require no fasting unless a lipid panel is ordered; just bring a medication list. For stool collection, use the kit provided, collect a small sample, keep it refrigerated, and deliver it to the lab within 24 hours.
What do common result ranges mean?
CRP < 5 mg/L is normal; 5‑10 mg/L suggests mild inflammation; > 10 mg/L often indicates an active flare. Fecal calprotectin < 50 µg/g is normal; 50‑200 µg/g may be mild disease; > 200 µg/g usually signals active IBD.
How often should I have biomarker testing done?
Most gastroenterologists recommend testing every 6‑12 months for stable disease, and sooner (e.g., every 1‑3 months) when adjusting medication, experiencing new symptoms, or tapering steroids.
Will my insurance cover these tests?
CRP is generally covered without prior authorization. Fecal calprotectin often requires a prior authorization or a specific order from a gastroenterologist. Check with your insurer and ask your provider for any necessary documentation.