Feeling like everyday tasks are a rollercoaster you didnt sign up for? Youre not alone. Most people with dysautonomia wonder, What can actually help my symptoms, and is it safe? The short answer: there are lifestyle tweaks, medications, and emerging therapies that can make a real difference, but the best plan is tailored to you.
In this guide, Ill walk you through the whole journeyfrom spotting redflag symptoms to choosing a treatment that balances relief with safety. Think of it as a friendly roadmap, not a medical textbook, and feel free to pause, take notes, or jump to the part that matters most right now.
Quick Treatment Checklist
What are the redflag symptoms that demand immediate medical attention?
If you experience sudden fainting, severe chest pain, or a rapid drop in blood pressure that leaves you feeling dizzy for more than a few minutes, call emergency services right away. Those signs can indicate that the autonomic system is struggling to keep you stable.
How quickly should you start dysautonomia treatment after diagnosis?
Ideally, start addressing the most troublesome symptoms within weeks of a confirmed diagnosis. Early interventionespecially with lifestyle changesoften reduces the need for higherdose medications later on.
Can lifestyle changes alone control dysautonomia?
For many, simple adjustments like increasing fluid intake, adding a pinch of salt, and wearing compression garments can dramatically cut down on dizziness and fatigue. However, if symptoms persist or worsen, medication may become necessary.
QuickReference Table SymptomsvsUrgency
| Symptom | Urgency | Recommended Action |
|---|---|---|
| Sudden fainting (syncope) | Immediate | Call emergency services |
| Persistent lightheadedness | High | See a specialist within days |
| Mild orthostatic dizziness | Moderate | Start lifestyle tweaks, track response |
Understanding Dysautonomia Diagnosis
How is dysautonomia diagnosed?
Doctors usually start with a detailed history and a physical exam, then move on to tests that evaluate heart rate and blood pressure changes when you stand up. The tilttable test is the gold standard, and autonomic function labs can pinpoint specific subtypes.
What tests does the NHS use for dysautonomia?
In the UK, the NHS typically offers a tilttable test, blood work to rule out anemia or thyroid issues, and sometimes a 24hour heartrate monitor. If youre in the US, you might also see a quantitative sudomotor axon reflex test (QSART) to gauge sweatgland function.
Is there an online Do I have dysautonomia? quiz thats reliable?
Many websites host selfassessment quizzes, but theyre best used as a conversation starter with your doctornot a definitive diagnosis. A reputable quiz will ask about symptoms like postural tachycardia, gastrointestinal upset, and temperature regulation problems.
Stepbystep Flowchart From Referral to Diagnosis
- Primarycare visit symptom checklist
- Referral to autonomic specialist tilttable test
- Blood/urine labs ruleout secondary causes
- Final diagnosis personalized treatment plan
Credible Sources
For deeper reading, the offers a comprehensive overview, and the UKs outlines the typical test pathway.
Core Treatment Pillars
Medication Options
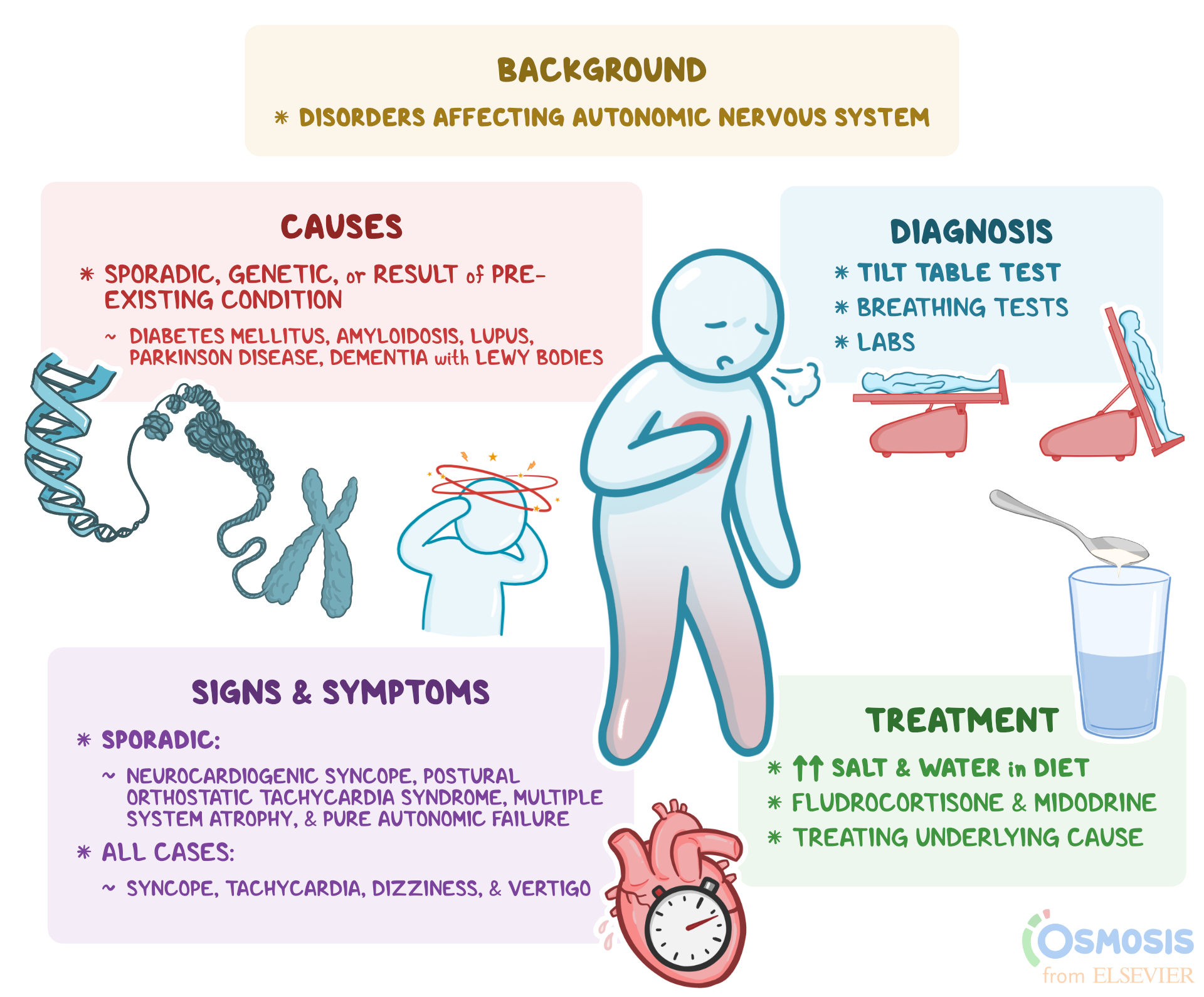
Medications are chosen based on which part of the autonomic nervous system is underperforming. Below are the most commonly prescribed classes:
Medication Comparison Table
| Drug | Primary Indication | Typical Dose | Common SideEffects | Evidence Rating* |
|---|---|---|---|---|
| Fludrocortisone | Low blood pressure | 0.1mg0.2mg daily | Fluid retention, hypertension | (Cleveland Clinic) |
| Midodrine | Orthostatic hypotension | 510mg three times daily | Piloerection, supine hypertension | (PubMed review) |
| Betablockers (e.g., propranolol) | Postural tachycardia | 2040mg twice daily | Fatigue, cold extremities | (clinical guidelines) |
| Ivabradine | Persistent tachycardia | 57.5mg twice daily | Bradycardia, visual disturbances | (recent trials) |
*Evidence rating reflects the amount and quality of peerreviewed research supporting each medication.
Lifestyle & SelfManagement
Think of lifestyle changes as the foundation of any treatment planlike a sturdy base for a house. Theyre inexpensive, lowrisk, and surprisingly effective when done consistently.
Practical DayintheLife Checklist
- Morning waterbolus: 500ml of plain water within 15minutes
- Saltrich breakfast: a pretzel, salted nuts, or broth
- Compression stockings (3040mmHg) for most of the day
- Small, frequent meals to avoid postprandial drops
- Gradual, seatedtostanding exercises (10minute sessions)
Procedural & Emerging Therapies
When standard meds and lifestyle tweaks dont fully control symptoms, some patients turn to newer interventions. These are usually offered at specialized centers and may be part of a clinical trial.
EmergingTherapy Summary
- Transvascular Autonomic Modulation (TVAM) a pilot study showed modest improvements in bloodpressure stability ().
- Neuromodulation devices implanted or wearable stimulators that target vagal pathways ().
- IV fluid therapy shortterm saline infusions for acute flares, especially in severe orthostatic intolerance.
Types of Dysautonomia
What is the firstline treatment for Postural Orthostatic Tachycardia Syndrome (POTS)?
POTS often responds well to a combination of increased fluids, 0.30.5g of salt per day, and lowdose betablockers or ivabradine. Physical reconditioningstarting with recumbent exerciseis also a cornerstone.
How is familial dysautonomia managed differently from other forms?
Because familial dysautonomia involves sensory and gastrointestinal dysfunction, treatment focuses on eye lubrication, gastrostomy feeding when needed, and medications that aid gastric motility (e.g., erythromycin).
What treatments are recommended for dysautonomia secondary to Parkinsons disease?
Midodrine and fludrocortisone are commonly used for orthostatic hypotension in Parkinsons patients, while adjusting dopaminergic therapy can help with heartrate variability issues.
MiniTable TypevsPrimary Treatment
| Type | Primary Treatment |
|---|---|
| POTS | Betablocker/Ivabradine + salt + fluids |
| Familial | Artificial tears, GI motility agents |
| Parkinsonrelated | Midodrine + fludrocortisone |
CaseStudy Box
Emily, a 28yearold with POTS, reduced her daily dizziness from almost every hour to once a week after adding a 500ml waterbolus each morning, wearing 30mmHg stockings, and starting lowdose propranolol. Her story shows how a few simple steps can cascade into big improvements.
Benefits vs Risks
What are the common sideeffects of dysautonomia medication?
Most drugs can cause fluid retention, supine hypertension, or mild fatigue. Its essential to monitor blood pressure both lying down and standing, and to keep an open line of communication with your prescriber.
How to monitor treatment effectiveness safely?
Keep a symptom diary: note time of day, posture, fluid/salt intake, and any medication changes. Compare standing BP and heartrate readings before and after each adjustment. If you notice worsening symptoms, alert your clinician within a week.
When does a treatment become too risky for a particular patient?
If a medication triggers severe hypertension while youre lying down, or if you develop swelling that doesnt subside, the risk outweighs the benefit. Always discuss dose adjustments or alternative drugs before stopping a prescription abruptly.
RiskBenefit Decision Tree
- Identify dominant symptom (e.g., dizziness)
- Start with lowrisk lifestyle changes
- If symptoms persist add the lowesteffective medication dose
- Reevaluate every 34 weeks; adjust or discontinue as needed
Finding Specialist Help
How to locate a clinician experienced in dysautonomia treatment?
Look for centers that list autonomic dysfunction or dysautonomia on their website. In the U.S., the Cleveland Clinics Dysautonomia Center and NYU Langones Autonomic Disorders Program are recognized leaders. In the UK, most major teaching hospitals have an autonomic unit, and the NHS provides a searchable directory.
What questions should you ask during the first appointment?
- Which subtype of dysautonomia do you think I have, and why?
- What lifestyle changes should I start right now?
- How will we track progress and sideeffects?
- Are there clinical trials I might be eligible for?
Where can you find reliable patientsupport resources?
Online communities such as offer peertopeer advice, while the American Brain Foundation provides educational webinars. Remember to verify any anecdotal advice with a medical professional.
Resource Directory (External Links)
- Cleveland Clinic Dysautonomia Center authoritative clinical guidance
- The Dysautonomia Project patient stories and practical tips
- American Brain Foundation research updates and funding opportunities
- NHS Dysautonomia page UKspecific pathways and contact information
Conclusion
Living with dysautonomia can feel like navigating a maze, but you dont have to go it alone. By understanding your symptoms, getting a clear diagnosis, and building a treatment plan that blends lifestyle tweaks, targeted medication, andwhen neededadvanced therapies, you can reclaim steadier days and brighter nights. The journey is personal, so stay curious, keep tracking what works, and lean on trusted specialists and supportive communities.
Whats your biggest challenge with dysautonomia? Share your thoughts below, or download our free symptomtracking worksheet to start experimenting with the strategies we discussed. Together, well keep moving forwardone step at a time.
Many patients with overlapping neurological conditions also look for help with specific rare disorders. If you or a family member are exploring treatment or coverage options for specialty therapies, resources for atypical Rett syndrome can be helpful reading it explains diagnostic features and care approaches that sometimes overlap with autonomic symptom management.
FAQs
What are the first steps in managing dysautonomia symptoms?
Begin with lifestyle changes: increase daily water (about 2–3 L), add 2–3 g of salt, wear compression garments, and adopt small, frequent meals to avoid post‑prandial drops.
How much salt and water should I consume daily for dysautonomia?
Most patients benefit from 2–3 g of extra salt (≈½–1 tsp) and 2–3 liters of fluid spread throughout the day, but exact amounts should be tailored with your clinician.
When is medication necessary for dysautonomia?
If lifestyle tweaks don’t relieve dizziness, low blood pressure, or rapid heart‑rate, a doctor may prescribe fludrocortisone, midodrine, beta‑blockers, or ivabradine based on your specific subtype.
Can exercise improve dysautonomia, and what type is recommended?
Yes. Start with recumbent activities—e.g., rowing, recumbent bike, or water aerobics—and gradually progress to seated and then upright exercises as tolerance improves.
Are there any new therapies for dysautonomia on the horizon?
Emerging options include transvascular autonomic modulation, wearable vagal neuromodulation devices, and short‑term IV fluid protocols being evaluated in early‑phase clinical trials.