If youve just heard the words adult acute lymphoblastic leukemia (ALL) and your mind instantly jumps to how long do I have?, youre not alone. In a nutshell, the overall 5year survival for adults with ALL hovers around3040%, but the picture changes dramatically depending on age, disease subtype (Bcell vsTcell), genetic markers, and how quickly you achieve remission.
Below youll find the numbers broken down, the key factors that tilt the odds, realworld stories that bring the data to life, and practical tools you can use today to talk confidently with your medical team. Think of this as a friendly cheatsheet you can keep handyno jargon, just clear, compassionate information.
Survival Snapshot Overview
What is the overall 5year survival rate for adults with ALL?
The most recent populationbased studies from North America and Europe report a 5year net survival of roughly 35% for all adults combined. When you pool data from the United Kingdom, Canada, and the United States, the range tightens to 3040%.
How does age change the outlook?
Age is the single strongest predictor. Younger adults tend to do far better than their older counterparts. Below is a concise breakdown:
| Age Group | 5Year Survival | Key Notes |
|---|---|---|
| 1524years | 7075% | Often treated with paediatricstyle regimens; excellent response rates. |
| 2540years | 4560% | Benefit from intensive chemotherapy and early transplant when indicated. |
| 4160years | 3040% | Higher comorbidity burden; more reliance on targeted therapies. |
| >60years | 1520% | Often highrisk cytogenetics; treatment limited by fitness. |
These numbers come from a 2023 collaborative analysis published by the International Cancer Benchmarking Partnership. also reports very similar agestratified figures.
What does complete remission actually mean for adults?
In the ALL world, complete remission (CR) means that the bonemarrow blast count falls below5% and there are no signs of disease in the blood or other organs. Importantly, modern labs can also measure minimal residual disease (MRD)a level of cancer cells under 0.01% that predicts longterm survival. Achieving MRDnegative status within the first month of therapy is a strong harbinger of a 5year survival >60%.
How reliable are these survival statistics?
Survival data are presented in two ways: observed survival, which looks at actual outcomes in a cohort, and net survival, which adjusts for deaths from other causes. The numbers above are net survival, which gives a cleaner picture of how the disease itself impacts life expectancy. Remember, statistics are averagesindividual results can be better or worse based on a host of personal factors.
Key Prognosis Factors
Subtype Matters Bcell vsTcell
About 7080% of adult ALL cases are Bcell lineage, while the rest are Tcell. Historically, Tcell ALL has a slightly lower survival rate, but newer frontline regimens have narrowed the gap.
| Subtype | Typical 5Year Survival | Distinct Features |
|---|---|---|
| Bcell ALL | 3545% | More likely to harbor the Philadelphia chromosome (BCRABL1); responds well to tyrosinekinase inhibitors. |
| Tcell ALL | 3035% | Often presents with a mediastinal mass; May benefit from nelarabinebased protocols. |
Genetics and Molecular Markers
Genetic abnormalities are the silent architects of prognosis. Here are the big players:
- Philadelphia chromosome (BCRABL1) once a grim sign, now treatable with drugs like imatinib, dasatinib, or ponatinib; 5year survival rises to about50% when these are added to chemotherapy.
- KMT2A (MLL) rearrangements highrisk, especially in younger adults; often require intensified therapy and transplant.
- iAMP21 another highrisk marker that pushes clinicians toward early transplant.
- Lowrisk cytogenetics (e.g., hyperdiploidy) associated with 5year survival >70% in the paediatrictype protocols applied to adults.
These associations are detailed in the National Cancer Institutes PDQ summary of adult ALL.
Treatment Variables
How the disease is tackled makes a massive difference:
- Induction intensity Paediatricstyle regimens (higher dose methotrexate, asparaginase) have improved adult outcomes, especially under 40years old.
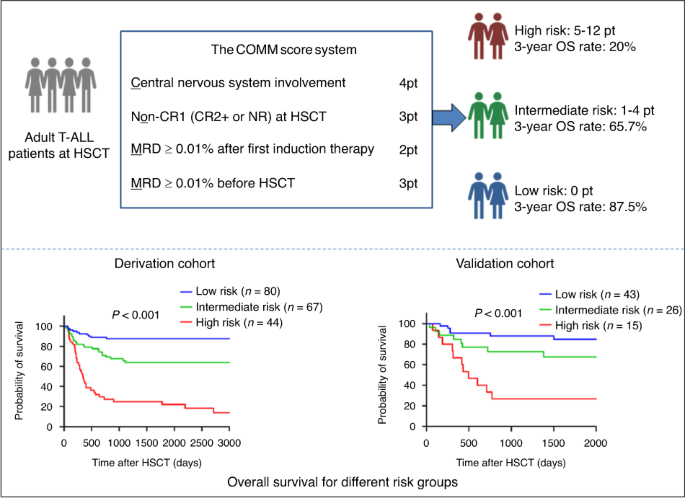
- Allogeneic stemcell transplant (SCT) For highrisk patients (e.g., MRDpositive after induction), SCT can lift 5year overall survival to around4550%.
- Targeted therapy Tyrosinekinase inhibitors for Phpositive disease, and emerging CART cell therapies for relapsed/refractory cases, have reshaped the survival curve in the last five years. More details about these advances can be found on the American Cancer Society website.
PatientSpecific Factors
Beyond the disease, the person matters. Consider these variables when you or a loved one sit down with the oncologist:
- Performance status (ECOG) A score of 01 (fully active) predicts better tolerance to intensive chemo.
- Comorbidities Diabetes, heart disease, or chronic lung problems can limit the aggressiveness of therapy.
- Socioeconomic support Access to a transplant centre, insurance coverage, and a strong support network are proven to improve adherence and outcomes.
- Lifestyle choices While quitting smoking or improving nutrition wont cure ALL, they can reduce treatment complications and improve overall wellbeing.
Patient Stories & Insights
Young adult who beat the odds
Meet Maya, a 32yearold graphic designer diagnosed with Bcell ALL in early 2022. Her bonemarrow biopsy showed a Philadelphia chromosome, but because she was otherwise healthy, she started a paediatrictype protocol plus dasatinib. Remarkably, she achieved MRDnegative remission after just three weeks.
I was terrified at first, Maya recalls, but my doctor explained the numbers in plain English. Knowing that an early MRDnegative result could push my 5year survival past 60% gave me a concrete goal to work toward. She completed a matchedsibling transplant a year later and is now celebrating five years diseasefree.
Oncologists perspective
Dr. Elena Ramirez, a hematologyoncologist at the Mayo Clinic, says, When patients ask how long can I live with leukemia without knowing?, the honest answer is that many cases are caught early enough that we can intervene before symptoms appear. Early detection, combined with modern targeted agents, has turned what used to be a terminal diagnosis into a chronic, manageable condition for many adults.
She adds, The numbers we share are not destiny. Theyre a roadmap. If you stay on trackmaintain fitness, keep appointments, and speak up about sideeffectsyou can shift your personal odds in a positive direction.
Practical Resources Guide
Prognosis calculators
Several reputable cancer centres host online calculators that let you input age, subtype, MRD status, and cytogenetics to see an individualized survival estimate. The tool, for example, updates its algorithm yearly based on the latest clinical trial data.
Support communities
Living with ALL is as much an emotional journey as a medical one. The Leukemia & Lymphoma Society runs virtual support groups, peermentor programs, and a library of patientauthored stories. Connecting with others who speak your languagewhether youre dealing with Bcell or Tcell diseasehelps diminish the feeling of isolation.
Financial & legal aid
Many hospitals have socialwork departments that can navigate insurance approvals for expensive targeted therapies or transplant costs. Additionally, charities such as offer limitedtime grants for medication copays.
Doctor Conversation Tips
Prepare your questions
Before your next appointment, write down the top three things you need clarified. Examples:
- What is my MRD status, and how does it affect my 5year prognosis?
- Are there any clinical trials that match my Bcell ALL profile?
- If my disease relapses, what are the nextline optionsCART, bispecific antibodies, or transplant?
Having a concrete list keeps the visit focused and ensures you leave with actionable information.
Request a copy of your pathology report
Understanding the exact genetic abnormalities (e.g., Phpositive, KMT2Arearranged) empowers you to discuss targeted therapies confidently. Ask the clinic to send you a plainlanguage summary if the technical report feels overwhelming.
Discuss lifestyle support
While lifestyle changes wont erase the disease, they can smooth the treatment journey. Suggest a referral to a nutritionist, a physicaltherapy program, or a mentalhealth counselorespecially if youre feeling anxious about the prognosis numbers.
Conclusion
Adult ALL prognosis is a mosaic painted with age, disease subtype, genetics, and the speed of treatment response. The average 5year survival sits around 3040%, yet younger patients or those who achieve early MRDnegative remission can see rates above 60%. By grasping the key factorsBcell vsTcell, cytogenetic risk, treatment intensity, and personal healthyou can turn abstract statistics into a clear, personalized roadmap.
Use the tools and tips above to ask informed questions, connect with supportive communities, and stay proactive about your care. Remember, numbers are guides, not verdicts; with the right team and a solid support system, your journey can be one of hope, resilience, and sometimes, a surprising bounceback.
FAQs
What is the overall 5‑year survival rate for adult ALL?
Across population‑based studies, adult acute lymphoblastic leukemia has a net 5‑year survival of roughly 30‑40 %.
How does age affect adult ALL prognosis?
Age is the strongest predictor: patients 15‑24 years old see 70‑75 % survival, while those over 60 years often have only 15‑20 %.
What is MRD and why is it important?
MRD (minimal residual disease) measures tiny amounts of leukemia cells (<0.01 %). Achieving MRD‑negative status early in treatment is linked to 5‑year survival rates exceeding 60 %.
Which genetic markers most influence adult ALL prognosis?
Key markers include the Philadelphia chromosome (BCR‑ABL1), KMT2A (MLL) rearrangements, iAMP21, and low‑risk cytogenetics such as hyperdiploidy. Each markedly alters survival expectations.
When is an allogeneic stem‑cell transplant recommended for adult ALL?
Transplant is advised for high‑risk patients—those with unfavorable genetics, MRD‑positive after induction, or relapsed disease—as it can raise 5‑year overall survival to about 45‑50 %.