Recognizing AML Early
What signs should make me think of leukemia during pregnancy?
Many pregnancyrelated changes can mask serious issues, but there are redflags that deserve a second look:
- Persistent, unexplained fatigue that doesnt improve with rest.
- Easy bruising or spontaneous bleeding from gums and nose.
- Night sweats or fevers that linger beyond a typical infection.
- Sudden drops in blood countsespecially platelets and hemoglobin.
If you notice two or more of these, ask your obstetrician for a complete blood count and, if needed, a peripheral smear. Early detection can be a gamechanger.
How do these symptoms differ from normal pregnancy changes?
| Symptom | Common in a healthy pregnancy? | Alarm signal for AML |
|---|---|---|
| Fatigue | Yes, especially first trimester | Severe, progressive, not relieved by rest |
| Bruising | Rare unless thrombocytopenia | Frequent, spontaneous, no clear cause |
| Gum bleeding | Rare | Possible leukemic infiltration |
| Elevated WBC & blasts | Possible with infection | Presence of blasts = strong AML indicator |
Having a concrete table like this can help you (and your doctor) decide whether further testing is warranted.
TrimesterBased Decisions
Why does the week of pregnancy matter for AML treatment?
Pregnancy isnt just a stateits a dynamic environment that changes every few weeks. Some drugs cross the placenta safely after the first trimester, while others are teratogenic throughout. The key is to match the aggressiveness of your leukemia with the safety window for the baby.
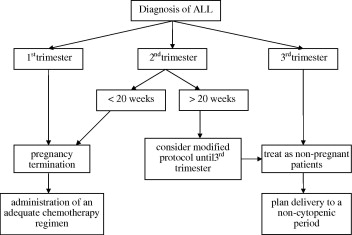
First Trimester: What are my options?
During weeks013, the embryo is most vulnerable. Antimetabolites like cytarabine carry a higher risk of birth defects. According to the , many hematologists consider one of two paths:
- Modified induction: Use an anthracyclineonly regimen (e.g., daunorubicin) to buy time while monitoring the disease closely.
- Pregnancy termination: For rapidly progressing AML where fulldose chemo is crucial, some patients choose termination to enable aggressive treatment without fetal risk.
Both routes are emotionally heavy, but involving a multidisciplinary teamhematology, maternalfetal medicine, and mentalhealth professionalshelps you make an informed, compassionate decision.
Second Trimester: Can I receive standard chemo?
From week14 onward, the placenta has matured enough that many standard regimens become safer. The recommends the classic 7+3 induction (daunorubicin + cytarabine) at full doses for most AML cases. The risk of major malformations drops dramatically, though youll still need close fetal monitoring (ultrasounds every 23 weeks, growth scans, and doppler studies).
For guidance on aggressive hematologic care during pregnancy and coordination with maternity services, many patients find resources on AML pregnancy treatment useful when discussing options with their team.
Third Trimester: Is delivery part of the plan?
When you hit week2830 and are in remission or have a solid response to induction, the focus often shifts to timing the birth. Many doctors aim for delivery around 3436weeksearly enough to continue consolidation therapy without jeopardizing the babys lung development. Steroids may be given to accelerate fetal lung maturity, and a neonatal team stands by for a smooth transition.
Treatment Options Overview
What does how I treat AML in pregnancy look like in practice?
Below is a quick rundown of the most common therapeutic pillars, tweaked for each trimester.
Standard Induction (7+3)
- Daunorubicin an anthracycline; considered relatively safe after the first trimester.
- Cytarabine an antimetabolite; used at full dose from week14 onward, reduced dose if youre still early.
Drug Safety by Trimester
| Drug | 1st Trimester | 2nd Trimester | 3rd Trimester |
|---|---|---|---|
| Cytarabine (antimetabolite) | High teratogenic risk | Moderate reduced dose or delayed until 14weeks | Generally safe at standard dose |
| Daunorubicin (anthracycline) | Limited data often used alone | Considered safe | Safe |
| ATRA (alltrans retinoic acid) | Contraindicated | Preferred for APML | Safe |
| Gemtuzumab ozogamicin | Insufficient data | Not recommended | May be considered in trials |
How is Acute Promyelocytic Leukemia (APML) different?
If your AML is the APML subtype, the game changes dramatically. The highrisk hemorrhagic profile of APML makes prompt treatment essential, yet many of the usual agents (like arsenic trioxide) are offlimits during pregnancy. The sweet spot is ATRA monotherapy during weeks1324, which drives the malignant cells to mature without the need for cytotoxic drugs. The shows excellent maternal remission rates and minimal fetal complications when ATRA is used alone in the second trimester.
Supportive Care: What else should I expect?
Chemo alone wont keep you and your baby safe. Youll likely need:
- Blood product transfusions to maintain platelets >2010/L and hemoglobin >8g/dL.
- Antimicrobial prophylaxisfluoroquinolones after the first trimester are considered safe.
- Close obstetric surveillanceweekly growth ultrasounds, amniotic fluid assessments, and fetal heart monitoring.
- Psychological counselingthe emotional burden can be huge; speaking with a therapist or a support group is vital.
APML Special Cases
Can I use ATRA safely in the second trimester?
Yes. The reports that women who received ATRA between weeks13 and24 achieved complete remission in >90% of cases, with no increase in major congenital anomalies. The key is to avoid adding arsenic trioxide or highdose chemotherapy until after delivery.
What about after delivery?
Once the baby is born, you can transition to the full APML protocolATRA plus arsenic trioxide or a standard ATRAbased consolidation. Neonatal care teams are prepared for any transient myelosuppression in the newborn if drug exposure occurred late in pregnancy.
Support & Resources
Where can I find reliable guidelines?
Both the and the maintain uptodate, peerreviewed guidelines on acute myeloid leukemia in pregnancy. Bookmark their PDF pagestheyre the gold standard for physicians and patients alike.
Which organizations help patients navigate this journey?
- Leukemia & Lymphoma Society offers patient navigation, financial aid, and counseling.
- Motherhood & Cancer Support Network a community of mothers who have faced cancer while pregnant.
- Local hospitals maternalfetal medicine unit most major cancer centers have a dedicated team that talks you through each step.
What about future pregnancies?
After achieving remission, many women wonder, Can I get pregnant again? The answer is generally yes, especially after a diseasefree interval of at least two years. Fertilitypreserving optionsegg or embryo freezingcan be discussed before initiating treatment. A fertility specialist familiar with oncology cases will help you map out a safe timeline.
Balancing Benefits and Risks
Every decision you makewhether to start fulldose chemo now, delay until the second trimester, or consider terminationcarries both potential benefits and risks. The most trustworthy path is transparent communication with a team that includes a hematologist, an obstetrician specialized in highrisk pregnancies, a neonatologist, and a mentalhealth professional. Ask them for data, not just opinions. Remember, youre not alone; countless women have walked this road, and the medical community continues to refine protocols that keep both mother and baby safe.
Conclusion
Treating AML while youre pregnant is undeniably tough, but its not hopeless. By recognizing early warning signs, appreciating how each trimester shapes treatment choices, and leveraging evidencebased regimens like anthracyclinebased induction or ATRA for APML, you can aim for remission without compromising your babys health. Lean on the reputable guidelines from ASH and BSH, connect with support organizations, and keep an open dialogue with your care team. You deserve clear, compassionate answersso ask questions, share your fears, and remember that a thoughtful, personalized plan is your strongest ally. If you have thoughts or experiences to add, feel free to write in the comments below; were all in this together.
FAQs
What are the first signs of AML that I should watch for during pregnancy?
Unexplained fatigue, easy bruising or bleeding, night sweats, persistent fevers, and a sudden drop in blood counts (especially platelets or hemoglobin) are red‑flags that merit a CBC and possibly a peripheral smear.
Can standard AML chemotherapy be given safely in the second trimester?
Yes. From about week 14 onward, the classic “7 + 3” induction (daunorubicin + cytarabine) is considered safe for the fetus, though close fetal monitoring is essential.
How is acute promyelocytic leukemia (APML) treated differently in pregnancy?
For APML, ATRA monotherapy is used in the second trimester (weeks 13‑24) because it induces remission without the need for cytotoxic drugs that may harm the baby.
What supportive care measures are needed while undergoing AML treatment in pregnancy?
Patients typically require blood product transfusions, antimicrobial prophylaxis, regular obstetric ultrasounds, and psychological counseling to address the emotional strain.
When is delivery usually planned for a pregnant woman who has responded to AML treatment?
If remission is achieved and the pregnancy is beyond 28‑30 weeks, doctors often aim for delivery around 34‑36 weeks to allow continuation of consolidation therapy while minimizing neonatal complications.