Wondering how likely cervical cancer is to come back and what that really means for you? In the next few minutes well break down the realworld outlook, the symptoms that matter, and the options you have right now. Whether the recurrence shows up after two years, five years, or even a decade, knowing the numbers and the next steps can give you the confidence to act fast.
Prognosis & Survival
Lets start with the hard numbers the ones that often feel overwhelming but are essential for planning.
Overall survival rates
When cervical cancer returns, the median overall survival (OS) generally falls between 7 and 12 months. A recent metaanalysis reported a fiveyear OS of less than 5% despite the best available therapies. The same study found a median survival of 1317 months for patients who received aggressive multimodal treatment.
Local vs. distant recurrence
Survival chances differ dramatically based on where the cancer reappears:
- Localonly recurrences (confined to the pelvis) can achieve longterm survival rates up to 30% after a pelvic exenteration, a complex but potentially curative surgery.
- Distant metastasis (spread to lungs, liver, or bones) typically sees a fiveyear survival around 17%**still low, but newer systemic therapies are slowly nudging the curve upward.
Key prognostic factors
Doctors look at several red flags when estimating outlook:
| Factor | Impact on Survival |
|---|---|
| Time to recurrence | Recurrence <2years poorer prognosis |
| Stage at original diagnosis | Higher stage (IB2, IIB) lower OS |
| HPV status | Persistent highrisk HPV higher risk of distant spread |
| Performance status | Better functional health more treatment options |
To keep the information trustworthy, I always crosscheck these figures with the latest and peerreviewed journals. For people exploring the impact of other cancers, including what happens after prostate removal life expectancy, similar principles about recurrence and survival rates apply: the earlier it's detected and properly treated, the better the long-term outcome in most cases.
Timing of Recurrence
When you hear recurrence, the first question is usually how soon? The timing actually guides how aggressive the next round of treatment can be.
Typical windows
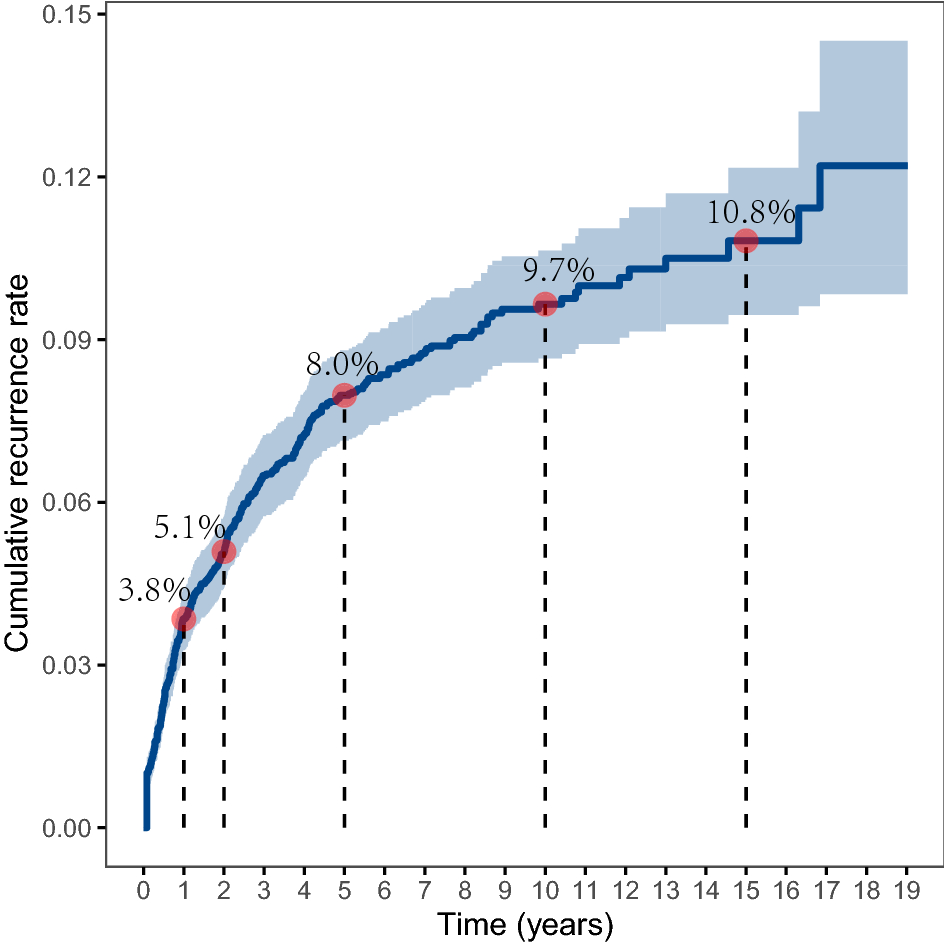
About 68% of recurrences happen within the first two to three years after the initial treatment. Breaking it down:
- Year1: roughly 3.8% of patients see cancer return.
- Year2: an additional 5.1%.
- Year3: another 8%.
Beyond five years
Even after the fiveyear cure mark, theres still a 510% chance of a late recurrence. Its rare, but it does happenespecially in patients who had highrisk features the first time around. And yes, a handful of case reports describe recurrences after 10years or more, reminding us that lifelong vigilance is never a bad idea.
Why timing matters
If the cancer reappears early, surgeons often have a better shot at removing it completely. Latestage recurrences, on the other hand, may be limited to systemic therapy or enrollment in a clinical trial. In short, the sooner we catch it, the more options we have. In fact, similar patterns are seen in other cancers, such as how early prostate cancer detection dramatically improves the likelihood of choosing the most effective treatments right from the start.
Warning Symptoms
Spotting a recurrence early can be a gamechanger. Below are the redflag signs that should prompt an immediate call to your oncology team.
General warning signs
- Unexpected vaginal bleeding or spotting.
- Persistent pelvic or lowerback pain that doesnt improve with usual pain relievers.
- Unexplained weight loss or loss of appetite.
- Newly foulsmelling discharge.
After a hysterectomy
If youve had a hysterectomy, the symptoms can feel a bit different because the uterus is gone. Look out for:
- Vaginal cuff tenderness or swelling.
- Watery or mucouslike discharge from the vaginal vault.
- Recurrent urinary urgency or frequency without infection.
Quick selfcheck
| Symptom | Frequency | Action |
|---|---|---|
| Any new bleeding | Any | Call oncologist within 48hrs |
| Pain lasting >2weeks | Often | Schedule urgent evaluation |
| Unusual discharge | Occasional | Get a pelvic exam ASAP |
Listening to your body is the first line of defensedont brush these signs off as just menopause or stress.
Treatment Options
When the cancer returns, the treatment landscape is a mix of triedandtrue methods and exciting new therapies. Heres a friendly rundown.
Standard approaches
- Pelvic exenteration a radical surgery that can achieve diseasefree survival in about 30%** of carefully selected patients.
- Radiation reirradiation often combined with chemotherapy to boost local control.
- Systemic chemotherapy platinumbased combos remain the backbone for distant disease.
- Immunotherapy pembrolizumab has earned FDA approval for PDL1positive recurrent cervical cancer, offering hope for a subset of patients.
Emerging therapies
Clinical trials are buzzing with innovative options:
- CART cell therapy targeting HPVrelated antigens.
- Therapeutic vaccines designed to train the immune system against residual cancer cells.
- Combination checkpoint inhibitors that aim to overcome resistance.
Checking clinicaltrials.gov for recurrent cervical cancer can reveal trials that might be a perfect fit for your situation. As research progresses, new evidence-based protocols are making headlines, for example, insights from promising turmeric cancer study results are being tested as supportive care in several centers, especially when patients are searching for complementary strategies.
Choosing the right path
The decision hinges on several personal factors: where the cancer returned, how well you tolerated previous treatment, your overall health, andperhaps most importantlyyour personal goals. A good oncologist will walk you through the pros and cons, helping you decide whether a bold surgical approach, a focused radiation plan, or a newer drug trial feels right for you.
Real Stories
Numbers are helpful, but stories bring them to life. Below are two anonymized experiences that illustrate the range of possibilities.
Case #1: StageIB2, early recurrence
Maria (33) finished chemoradiation for a stageIB2 tumor and thought she was in the clear. Six months later, she noticed occasional spotting. Imaging revealed a small pelvic nodule. Because the recurrence was localized and she was otherwise healthy, her team performed a pelvic exenteration. Today, four years later, Maria is cancerfree and volunteers with a survivor network, sharing that early detection saved her.
Case #2: Late recurrence after 9years
James (58) had a radical hysterectomy for stageIIA disease a decade ago. He felt fine for years, then started experiencing vague lowerback pain and a gradual loss of appetite. A PET scan uncovered metastatic lesions in the lungs. He enrolled in an immunotherapy trial that combined pembrolizumab with a novel vaccine. While the disease is still present, his tumor has shrunk considerably, and he says the hope from the trial keeps him fighting.
Takeaway lessons
- Early followup can catch a recurrence when curative surgery is still an option.
- Even very late recurrences can be managed with modern systemic therapies.
- Emotional supportwhether from friends, support groups, or online communitiesmakes a tangible difference in coping.
Balancing Risks
Every treatment carries potential benefits and sideeffects. Lets weigh them side by side so you can make an informed, balanced decision.
Benefits of aggressive therapy
- Potential for longterm remission, especially with localized disease.
- Psychological boost of doing everything possible.
Drawbacks and qualityoflife concerns
- Pelvic exenteration can lead to permanent colostomy and urinary diversionlifechanging adjustments.
- Radiation reirradiation may cause bowel toxicity, fatigue, or skin changes.
- Systemic therapies, while less invasive, can bring nausea, neuropathy, or immunerelated side effects.
Shared decisionmaking tools
Many cancer centers provide printable checklists that prompt you to ask about:
- Survival benefit estimates.
- Impact on daily activities.
- Support services (nutrition, counseling, rehab).
Using a structured worksheet helps keep the conversation focused on what truly matters to you.
Support Resources
Facing recurrence can feel isolating, but you dont have to walk this path alone.
Patientfocused organizations
- National Cancer Institute (NCI) uptodate information and clinical trial listings.
- American Cancer Society free counseling hotlines and survivorship guides.
- Cervical Cancer Alliance peerto-peer support groups, both online and inperson.
Financial and logistical help
Many hospitals have social workers who can assist with insurance appeals, transportation vouchers, and copay assistance programs. Dont hesitate to ask for a referral; these services are often underutilized.
Followup schedules
A typical surveillance plan after treatment includes:
- Physical exam and pelvic imaging every 34months for the first two years.
- Then every 6months until year5.
- Annual checkups after five years, with continued attention to any new symptoms.
Keeping a simple calendareither on your phone or a paper plannercan ensure you never miss an appointment.
Key Takeaways
Recurrent cervical cancer carries a sobering outlookmedian survival 712months and fiveyear overall survival under 5%but early detection, individualized treatment, and robust support can improve both length and quality of life. Stay vigilant for warning signs, keep the conversation open with your care team, and lean on trusted resources and survivor stories. If you or a loved one are navigating a recurrence, schedule that followup today, explore the treatment options that fit your goals, and remember youre not alone in this journey.
FAQs
What is the typical survival rate after recurrent cervical cancer?
Median overall survival is usually 7‑12 months, with a five‑year overall survival of less than 5 %; however, aggressive multimodal treatment can extend median survival to 13‑17 months.
When are recurrences most likely to happen?
About 68 % of recurrences occur within the first two‑three years after initial treatment, with the highest risk in the first two years.
Which symptoms should prompt an immediate doctor’s call?
Any new vaginal bleeding, persistent pelvic or lower‑back pain, unexplained weight loss, or foul‑smelling discharge should be reported to your oncologist within 48 hours.
What treatment options are available for a recurrence?
Standard options include pelvic exenteration, re‑irradiation with chemotherapy, systemic platinum‑based chemotherapy, and pembrolizumab for PD‑L1‑positive disease. Emerging therapies involve CAR‑T cells, therapeutic vaccines, and novel checkpoint‑inhibitor combinations.
How can I find clinical trials for recurrent cervical cancer?
Visit clinicaltrials.gov and search for “recurrent cervical cancer” to see eligibility‑based studies and newer experimental treatments.