



If leukemia spreads to the brain or spinal cord, you might start feeling headaches, seizures, blurry vision, facial numbness, or a sudden weakness in an arm or leg. Those are the central nervous system leukemia symptoms that act like an alarm bell, urging you to get checked right away. Catching them early can shave weeks off the diagnostic timeline and, honestly, can make a world of difference in treatment success.
Lets walk through whats going on, why it matters, and how you can stay one step ahead. Ill share the science, sprinkle in a few reallife stories, and keep things friendlylike a chat over coffee.
Overview of CNS Involvement
What is CNS leukemia?
CNS leukemia, sometimes called leukemia in the brain, occurs when leukemic cells breach the protective barriers of the central nervous system (CNS) and settle in the meninges, spinal fluid, or even brain tissue. Its not a separate disease; its a complication of the underlying blood cancer, most commonly seen in acute myeloid leukemia (AML) and acute lymphoblastic leukemia (ALL).
Risk categories (CNS1, CNS2, CNS3)
Doctors classify patients using the cns1 2 3 leukemia system based on how many leukemic blasts appear in the cerebrospinal fluid (CSF). Roughly:
- CNS1: No blasts in CSF.
- CNS2: A few blasts but not enough to meet the CNS3 threshold.
- CNS3: Significant blasts (5cells/L) or clinical signs of CNS disease.
Patients in the CNS3 group are at the highest risk for severe all cns involvement symptoms, and they often need more aggressive .
Key Warning Symptoms
Redflag symptoms you shouldnt ignore
| Symptom | Typical presentation | Why it happens | |||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Persistent headache | Feels like pressure, worsens when lying down | Increased intracranial pressure from leukemic infiltration | |||||||||||||||||||||||||||||||||||||
| Newonset seizures | Convulsions, possible loss of consciousness | Irritation of cortical tissue by malignant cells | |||||||||||||||||||||||||||||||||||||
| Vision changes | Double vision, blurry spots, loss of peripheral sight | Opticnerve or cranialnerve VI palsy | |||||||||||||||||||||||||||||||||||||
| Cranialnerve deficits | Facial numbness, hearing loss, trouble swallowing | Direct nerve compression or infiltration |
| Symptom | Typical presentation | Why it happens |
|---|---|---|
| Persistent headache | Feels like pressure, worsens when lying down | Increased intracranial pressure from leukemic infiltration |
| Newonset seizures | Convulsions, possible loss of consciousness | Irritation of cortical tissue by malignant cells |
| Vision changes | Double vision, blurry spots, loss of peripheral sight | Opticnerve or cranialnerve VI palsy |
| Cranialnerve deficits | Facial numbness, hearing loss, trouble swallowing | Direct nerve compression or infiltration |
| Motor weakness or numbness | Onesided weakness, tingling, pinsandneedles | Spinal cord or nerveroot involvement |
| Altered mental status | Confusion, lethargy, mood swings | Diffuse CNS involvement |
These symptoms cover the majority of leukemia in brain symptoms that patients report. If you notice any of them, especially in combination, its time to call your oncology team.
Symptoms by leukemia type
In AML with CNS involvement, headaches and seizures dominate the picture, while ALL patients more often present with cranialnerve palsieslike double vision or facial numbness. Thats why doctors ask very specific questions about visual changes and motor function during each visit.
Realworld snippet
John, a 42yearold with AML, suddenly experienced a seizure while cooking dinner. Hed also been battling a dull headache for a week. A lumbar puncture confirmed cns3 leukemia. After a series of intrathecal methotrexate treatments, his seizures stopped within two weeks and his headaches eased dramatically. Stories like Johns remind us that early recognition of central nervous system leukemia symptoms can change the trajectory of the disease.
How Leukemia Affects the Nervous System
Pathways of invasion
Leukemic cells travel to the CNS mainly via three routes:
- Hematogenous spread: Through the bloodstream, crossing the bloodbrain barrier.
- Meningeal seeding: Directly entering the protective layers surrounding the brain and spinal cord.
- Direct infiltration: Growing into brain tissue itself, which is rarer but more severe.
Understanding helps clinicians anticipate which symptoms might surface first and tailor imaging or CSF studies accordingly.
Diagnosing CNS Involvement
Key tests youll undergo
When a doctor suspects CNS disease, the goto tools are:
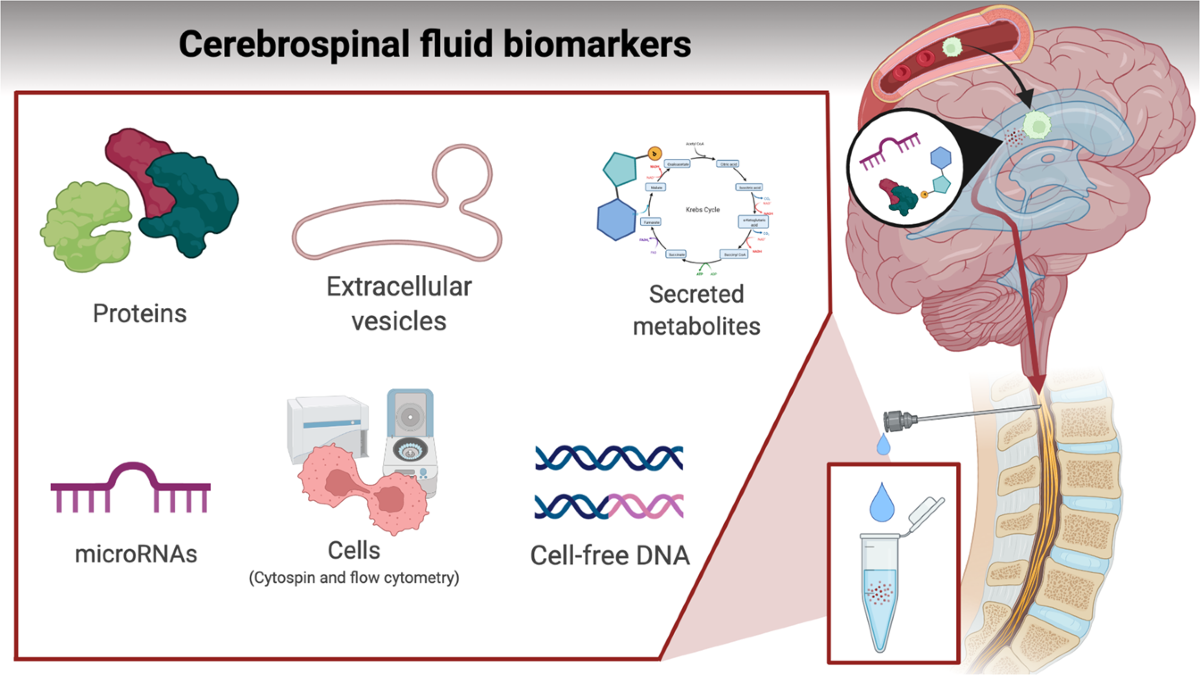
- Lumbar puncture (spinal tap): Collects CSF for cytology and flow cytometry to detect blasts.
- MRI of brain and spine: Highlights any lesions, leptomeningeal enhancement, or spinal cord compression.
Both tests are usually done promptly after the first red flag appears, because delaying diagnosis can let the disease progress silently.
Stepbystep diagnostic algorithm
Heres a quick roadmap you might see on your clinics whiteboard:
- Patient reports central nervous system leukemia symptoms Immediate neurological exam.
- Abnormal exam or concerning history Order MRI.
- MRI suggests involvement or symptoms are highrisk Perform lumbar puncture.
- CSF positive for blasts Classify as CNS1/2/3 and start cns leukemia treatment.
When to Seek Help
Urgent redflag checklist
If any of the following appear, treat them like a fire alarmdont wait:
- Severe or worsening headache that doesnt respond to usual meds.
- Any seizure, even if its just a brief spell.
- Sudden vision changes (double vision, loss of sight).
- New facial numbness, weakness in an arm/leg, or trouble speaking.
- Rapid changes in mental statusconfusion, drowsiness.
Call your oncologist, go to the emergency department, or have a trusted family member drive you. Early intervention can dramatically improve the cns leukemia survival rate.
Treatment Options Overview
Standard CNSdirected therapies
Two pillars dominate modern care:
- Systemic chemotherapy (the big guns that tackle disease throughout the body).
- Intrathecal chemotherapydrugs injected directly into the CSF (methotrexate, cytarabine, or a combination).
In some highrisk cases, physicians add cranialspinal radiation to the mix.
Comparison of treatment regimens
| Regimen | Typical Use | Response Rate | Key Side Effects |
|---|---|---|---|
| Systemic chemo + intrathecal MTX | Standard for AML & ALL with CNS disease | ~7080% remission in CNS3 patients | Mucositis, neurotoxicity (rare) |
| Systemic chemo + intrathecal cytarabine | Often used when methotrexate intolerance occurs | Similar remission rates | Myelosuppression, chemical meningitis |
| Systemic + intrathecal + cranialspinal RT | Reserved for refractory or bulky CNS disease | Higher local control, but mixed overall survival | Neurocognitive decline, fatigue |
Special note: AML with CNS involvement
When you hear aml with cns involvement treatment, think of an intensified schedule of intrathecal methotrexate combined with highdose cytarabine. Recent studies suggest that adding a targeted FLT3 inhibitor (if the patients leukemia carries that mutation) can improve the cns leukemia survival rate without substantially raising toxicity.
Survival Outlook Summary
Numbers youll see
Overall, the cns leukemia survival rate has climbed over the past decade thanks to better intrathecal regimens and early detection. Rough figures:
- CNS1: 5year survival mirrors systemic disease (7080%).
- CNS2: Slight dip (6070%).
- CNS3: Historically lower (4555%), but modern protocols push many patients into longterm remission.
When asked about leukemia in brain survival rate, the answer isnt a single numberit depends on age, leukemia subtype, and how quickly treatment begins. Early recognition of symptoms is the single most actionable factor you can control.
Managing Symptoms Daily
Practical tips for comfort
Even with aggressive therapy, symptoms can linger. Here are some downtoearth strategies that patients report helping:
- Headache control: Rotate acetaminophen and ibuprofen (if platelet counts allow); a cool compress on the forehead can be soothing.
- Seizure precautions: Keep a seizure diary, wear a medical alert bracelet, and have a rescue medication plan with your neurologist.
- Vision care: Use highcontrast glasses, limit screen time, and schedule regular ophthalmology checks.
- Mobility support: Gentle physiotherapy, balance exercises, and a sturdy walking aid can prevent falls if weakness appears.
- Mental health: Talk therapy, mindfulness apps, and leaning on support groups keep the emotional load lighter.
When to adjust treatment
If side effects become intolerablepersistent chemical meningitis after intrathecal therapy, severe neurocognitive changes, or uncontrolled infectionsyour doctor may pause intrathecal dosing or switch to a different agent. The goal is always to keep the disease under control while preserving quality of life.
Trusted Resources & Support
Finding reliable information can feel like searching for a needle in a haystack. Here are a couple of sources I trust and recommend:
- The provides uptodate clinical guidelines on CNS leukemia management.
- The offers patientfocused education, support groups, and financial aid resources.
Remember, no website can replace a conversation with your oncologist. Use these tools to ask informed questions and feel empowered.
Conclusion
Seeing central nervous system leukemia symptoms as a warning sign rather than a surprise can shave crucial weeks off the diagnostic process and boost your chances of a successful outcome. Headaches, seizures, vision changes, facial numbness, or sudden weakness are the bodys way of saying, Hey, somethings up in the brain or spine. Early detection, prompt diagnostic workup, and aggressive cns leukemia treatmentoften a mix of systemic chemo, intrathecal drugs, and sometimes radiationhave lifted the cns leukemia survival rate dramatically in recent years.
Stay vigilant, keep a symptom journal, and dont hesitate to reach out to your care team at the first hint of trouble. Youre not alone on this journeylean on trusted resources, connect with fellow warriors, and remember that knowledge truly is power. If you have questions or want to share your own experience, feel free to reach out. Together, we can navigate the complexities of CNS leukemia with confidence and compassion.
For patients worried about treatment options during pregnancy, see guidance on AML pregnancy treatment which discusses balancing maternal and fetal safety when CNS involvement coincides with pregnancy.
FAQs
What are the most common central nervous system leukemia symptoms?
Common symptoms include persistent headaches, seizures, vision changes, facial numbness, weakness in limbs, and altered mental status.
Can central nervous system leukemia cause vision problems?
Yes, vision changes such as double vision, blurry spots, or loss of peripheral sight can occur due to optic nerve or cranial nerve involvement.
Are seizures a sign of central nervous system leukemia?
Yes, new-onset seizures can be a warning sign of central nervous system leukemia, especially if accompanied by other neurological symptoms.
How is central nervous system leukemia diagnosed?
Diagnosis typically involves a neurological exam, MRI of the brain and spine, and a lumbar puncture to check for leukemic cells in the cerebrospinal fluid.
What should I do if I notice central nervous system leukemia symptoms?
If you experience symptoms like severe headache, seizures, vision changes, or sudden weakness, contact your oncology team immediately for prompt evaluation.

NHL Symptoms: Spot the Signs Early and Take Action
Recognize NHL symptoms like painless lumps, night sweats, and fatigue. Know when to see a doctor for non-Hodgkin lymphoma.
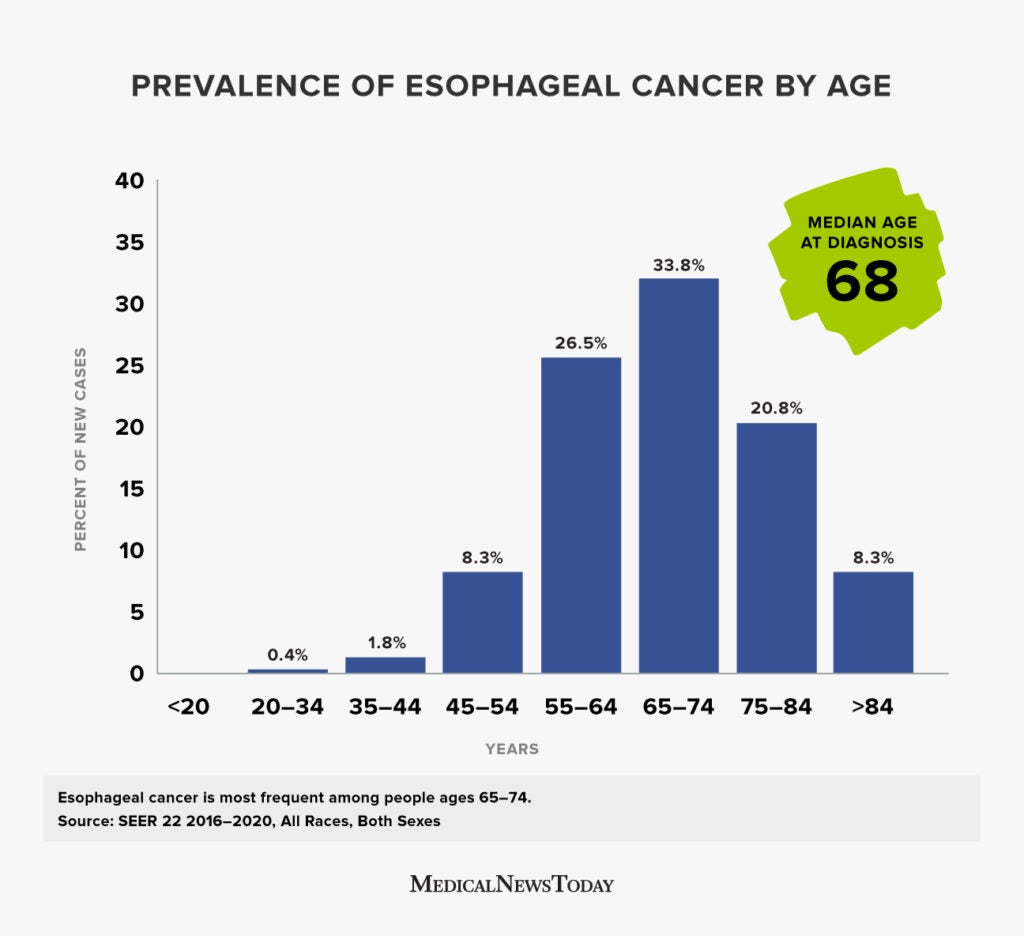
Esophageal Cancer at Age 40: Risks, Stats & Real Stories
Esophageal cancer at age 40 is rare but possible. Learn about symptoms, survival rates, and real stories for those diagnosed young.
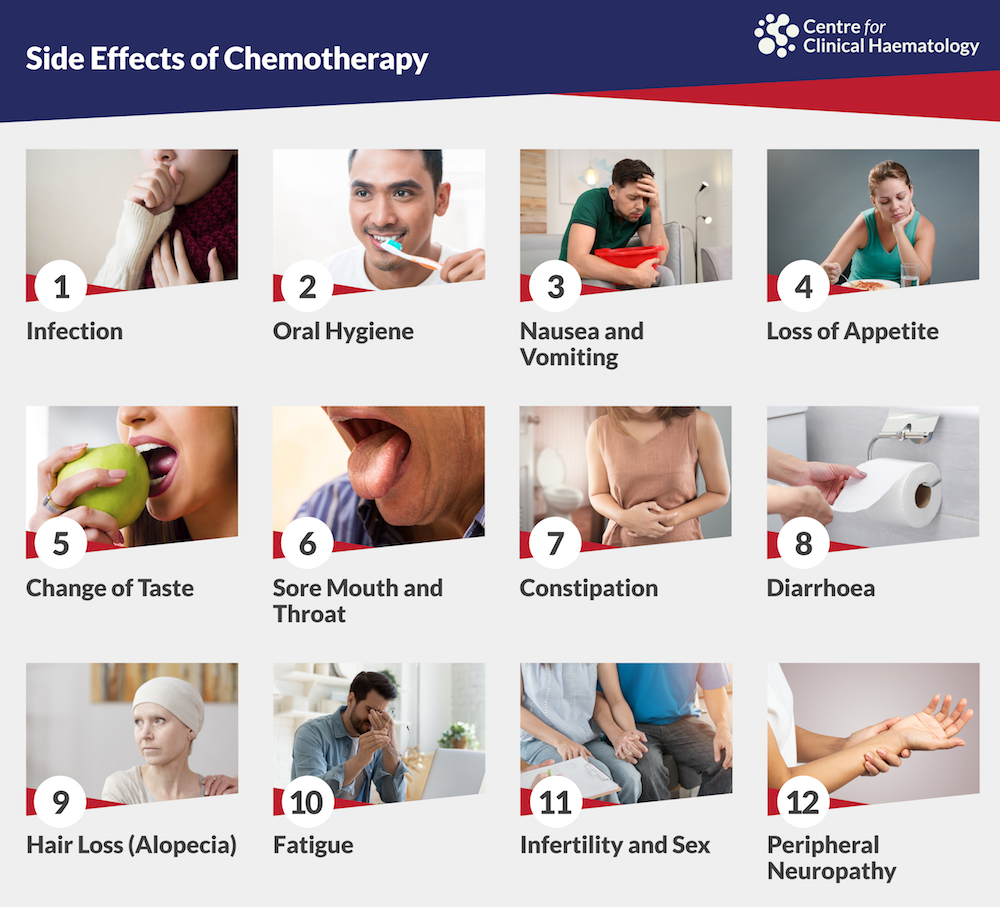
Symptoms of Second‑Hand Chemotherapy Exposure
Learn about secondhand chemotherapy exposure symptoms including rashes, nausea, and headaches. Protect yourself with proven safety precautions.
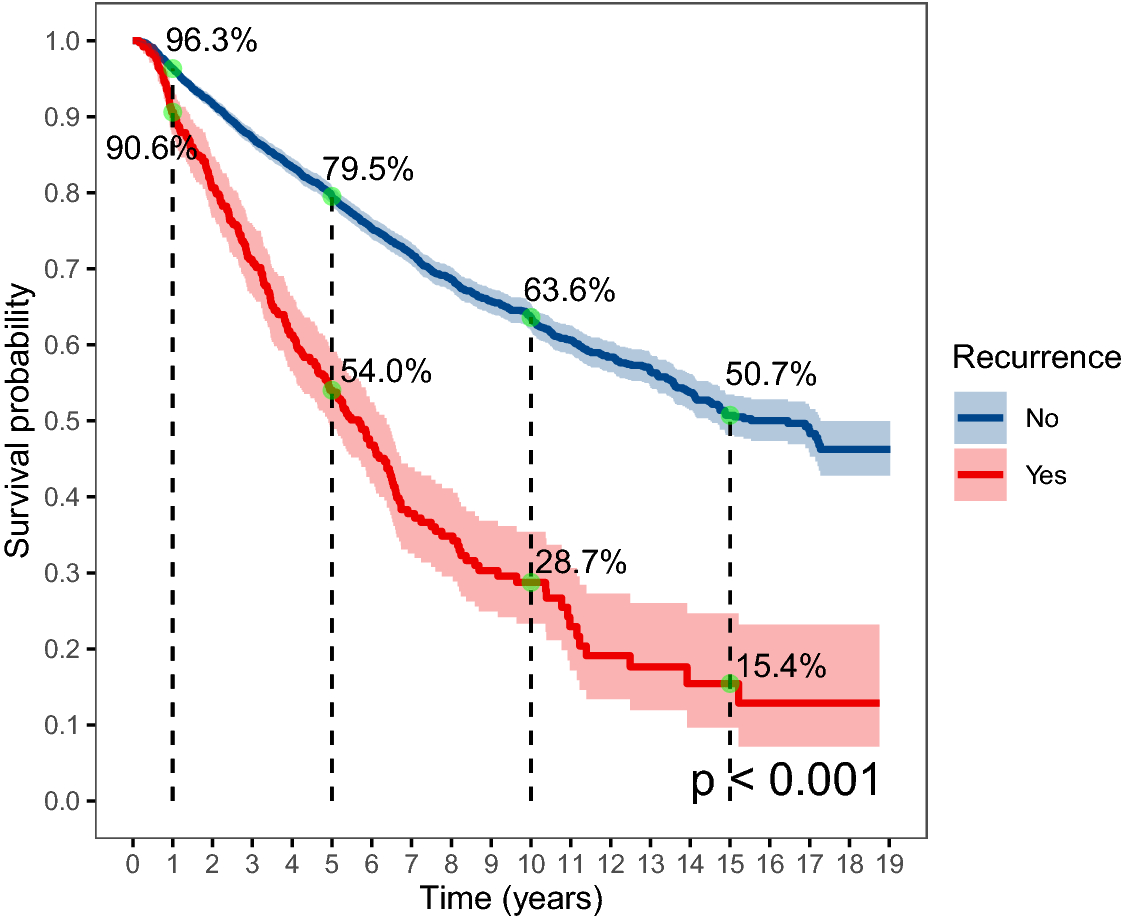
Understanding Recurrent Cervical Cancer: Hope & Options
Guidance on recurrent cervical cancer: warning signs, realistic survival outlook, and current treatment options for improved care.

Oral Cancer Types: What They Are and How to Spot Them
Oral cancer types show signs—persistent sores, patches, or lumps—so early detection can lead to faster treatment and survival.

FIGO Staging Cervical Cancer Radiology: Quick Guide
Quick guide to FIGO staging cervical cancer radiology, covering MRI, CT, PET‑CT roles, updates since 2018, and practical staging workflow.

Peritoneal Carcinoma: Symptoms, Stages, Treatment & Hope
Peritoneal carcinoma causes, stages, and treatment options explained. Get clear info on survival, symptoms, and expert care for peritoneal carcinoma.
Cholangiocarcinoma Diet: Simple, Nutritious Choices
A low‑fat, nutrient‑dense cholangiocarcinoma diet can help maintain weight, reduce side‑effects, and boost energy during treatment.

Monjuvi Strength: Dosage, Benefits, and Risks Explained
Monjuvi strength is 200 mg per vial, dosed at 12 mg/kg. Dosing calculations, infusion tips, benefits, risks, and patient advice.

Abdominal lymphoma survival rate: what you need to know
Abdominal lymphoma survival rate averages 80% at 5 years, reaching 90%+ for early MALT gastric types. Age, stage and treatment like RCHOP boost outcomes significantly for better prognosis.