Quick Summary Answer
Because Parkinsons disrupts the braintobowel signals that keep everything moving smoothly, many people with the disease experience bowel incontinence. The good news is that a mix of diet tweaks, safe laxatives, pelvicfloor exercises, and speciallydesigned incontinence products can bring back control and confidence.
Parkinsons and Bowel
What is bowel incontinence?
Bowel incontinence means the inability to hold stool (or gas) until you reach a bathroom. It can range from occasional leaks of gas to unexpected toilet accidents. The condition is distressing, but its also treatable.
Why does Parkinsons cause it?
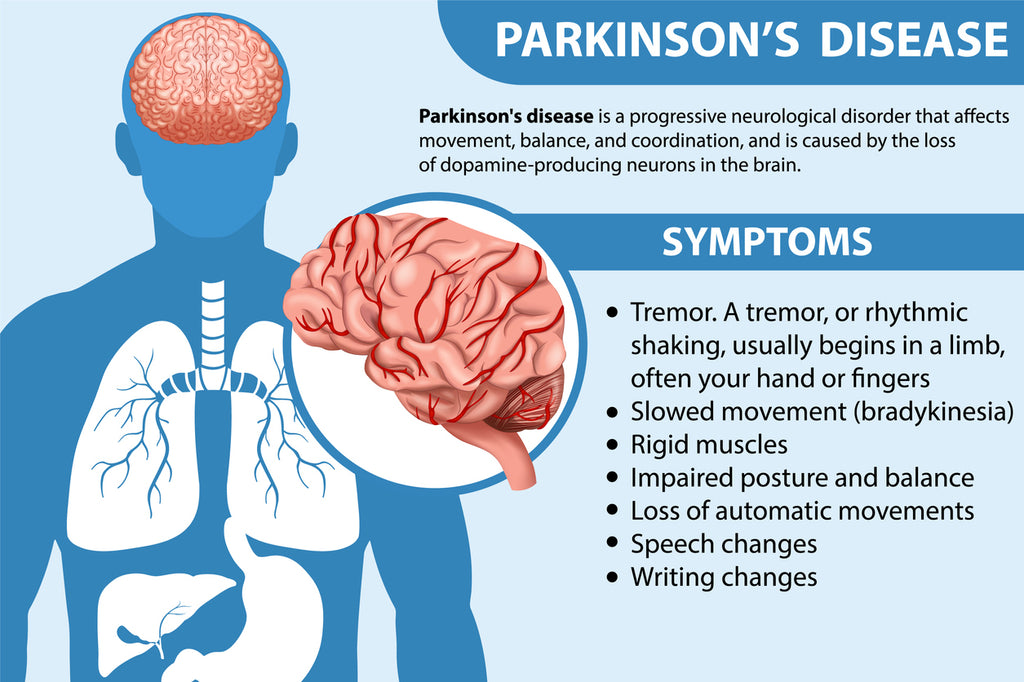
Parkinsons isnt just a movement disorder. The disease affects the autonomic nervous system, which governs the muscles of the colon and anal sphincter. When dopamineproducing neurons die, the coordination between the brain, colon, and pelvic floor weakens. Add in reduced mobility, medication side effects, and constipation, and the stage is set for accidental leakage.
How common is it?
Studies from the estimate that up to 40% of people with Parkinsons experience some form of bowel incontinence, especially in the midtolate stages of the disease. The risk climbs as rigidity and tremor affect the muscles needed for a reliable hold.
Common Bowel Symptoms
Loose bowels and diarrhea
Parkinsons and loose bowels is a frequent complaint. Medications like levodopa can speed up gut motility, while others (anticholinergics) may slow it down, creating a seesaw effect. Diarrhea can be triggered by a sudden increase in dopamine activity, making the colon contract too fast.
Constipation leading to leakage
Paradoxically, chronic constipation can cause overflow incontinence. Hard stool sits in the rectum, stretching the walls and weakening the sphincter. When softer stool finally passes, the weakened muscles cant hold it, resulting in sudden leaks.
Urine smell changes (quick FAQ)
While Parkinsons urine smell isnt directly linked to bowel issues, some people notice a stronger odor because of dehydration or medication metabolites. Keeping hydrated helps both urine and stool consistency.
How Doctors Diagnose
Symptom diary first
Before any tests, clinicians ask you to log bowel movements, diet, fluid intake, and medication timing for at least two weeks. This diary reveals patterns that point to neurogenic causes rather than a simple irritation.
Physical exam and manometry
A gentle rectal exam checks sphincter tone. If the tone feels low, an anorectal manometry may be ordered. This test measures pressure inside the anal canal while you squeeze, giving a clear picture of muscle strength.
When labs and imaging help
If blood tests show infection or inflammation, or if a colonoscopy reveals structural problems (like diverticulosis), doctors can rule out other sources of incontinence. Most of the time, the diagnosis rests on the neurological link.
Effective Treatment Options
Lifestyle and dietyour first line of defense
Highfiber foods (oats, berries, legumes) add bulk, while staying wellhydrated keeps stool soft. Aim for 2530g of fiber a day and at least eight glasses of water. A small trick: sipping warm lemon water first thing in the morning can stimulate colon activity.
What is the best laxative for Parkinsons?
Osmotic laxatives like polyethylene glycol (PEG) are usually safest because they draw water into the colon without causing strong cramps. Stimulant laxatives (senna, bisacodyl) work, but they can trigger cramping that mimics the tightmuscle symptoms of Parkinsons. Always start low and ask your pharmacist to doublecheck interactions with levodopa.
Pelvicfloor therapy and biofeedback
Specialized physical therapists teach you how to engage the pelvic floor correctly. Biofeedback devices give instant visual cuesthink of it as a video game for your sphincter, helping you rebuild strength and timing.
Medication tweaks for neurogenic incontinence
Anticholinergic drugs can relax a hyperactive bladder, but they may worsen constipation, so theyre used cautiously. Newer agents like mirabegron (a 3 adrenergic agonist) improve bladder storage without the constipating side effect, and they sometimes help the bowel too. Always discuss these options with a neurologist.
Incontinence productsno shame in protection
Theres a market of Parkinsons incontinence products designed for neurogenic leakage: highabsorbency briefs, absorbent pads with odorcontrol layers, and even disposable anal plugs. Look for products labeled highabsorbency and comfort waistband to avoid skin irritation.
Advanced interventions (rare)
For the stubborn few, sacral nerve stimulation or Botox injections into the anal sphincter can restore control. Surgery (e.g., sphincteroplasty) is a last resort, reserved for severe, refractory cases.
| Option | How it works | Typical Use | Common Side Effects | Cost/Access |
|---|---|---|---|---|
| Fiber diet | Adds bulk, softens stool | All stages | Gas, bloating | Low |
| PEG laxative | Osmotic water draw | Mildmoderate constipation | Diarrhea if overused | Lowmoderate |
| Pelvicfloor PT | Muscle retraining | Incontinence, poststroke | Initial discomfort | Moderate (insurance often covers) |
| Mirabegron | Relax bladder muscle | Urinary leakage | Hypertension, headache | Moderatehigh |
| Highabsorbency briefs | Physical barrier | All stages | Skin irritation if not changed | Lowmoderate |
Daily Management Tips
Timing meals with meds
Levodopa peaks about an hour after a meal. Plan highfiber breakfasts at the same time you take your morning dose, then give your gut a gentle kickstart. This sync reduces unexpected leaks later in the day.
Travel and social life hacks
Carry a small toilet kit: a few extra incontinence pads, wet wipes, and a discreet absorbent liner that fits into most regular underwear. Many cafs now have accessible restroomsdont be shy about asking.
Emotional support matters
Its completely normal to feel embarrassed. Joining an online community like the lets you hear real stories and discover tricks that arent in the textbooks. Sharing a laugh over a whoops moment can turn shame into solidarity.
Quickscan My Daily Bowel Plan
- Morning: Take levodopa, eat fiberrich oatmeal, drink a glass of water.
- Midday: Light walk (10min) to aid colonic transit.
- Afternoon: Check symptoms diary; if loose stool, sip electrolytes.
- Evening: Light dinner, avoid caffeine; consider a PEG dose if needed.
- Night: Use a breathable incontinence brief; change before bed.
Helpful Support Resources
For deeper dives, check out these trusted outlets:
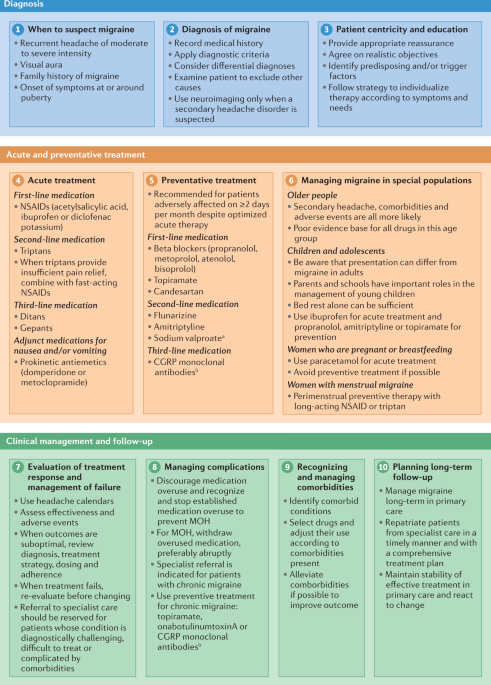
- headache assessment steps practical guides on structured symptom assessment that can be adapted to bowel symptom diaries.
- Bladder & Bowel Community peertopeer support forums.
- Stanford Medicines neurogastroenterology clinic offers telehealth pelvicfloor sessions.
Wrapping Up Summary
Living with bowel incontinence and Parkinsons can feel like navigating a maze blindfolded, but youre not alone. Understanding why the braingut connection falters, spotting the warning signs early, and using a toolbox of diet, medication, therapy, and protective products can restore a huge chunk of your independence.
Take the first step today: start a simple symptom diary, chat with your neurologist about a safe laxative, and explore one reputable incontinence product. Small changes add up, and every improvement is a win worth celebrating.
What strategies have helped you or a loved one? Share your experience in the commentsyour story might be the very tip someone else needs right now.
FAQs
What causes bowel incontinence in Parkinson’s disease?
Parkinson’s disease disrupts the communication between the brain, colon, and pelvic floor muscles due to the loss of dopamine-producing neurons, weakening muscle coordination and control over bowel movements.
How common is bowel incontinence among people with Parkinson’s?
Up to 40% of individuals with Parkinson’s experience bowel incontinence, especially during the mid to late stages of the disease when muscle rigidity and tremors worsen control.
What treatments help manage bowel incontinence in Parkinson’s?
Treatment often includes dietary changes to increase fiber and hydration, use of osmotic laxatives, pelvic floor physical therapy, medication adjustments, and specialized incontinence products.
Can constipation worsen bowel incontinence in Parkinson’s patients?
Yes, chronic constipation can cause overflow incontinence where hard stool weakens the anal sphincter, leading to leakage of softer stool.
Are there advanced treatment options for severe bowel incontinence in Parkinson’s?
For refractory cases, interventions like sacral nerve stimulation, Botox injections into the anal sphincter, or surgery such as sphincteroplasty may be considered.