Normaltension glaucoma (NTG) is a sneaky form of glaucoma where the optic nerve gets damaged even though eye pressure stays within the normal range. In plain English: you can lose part of your peripheral vision without the classic highpressure warning sign.
Below well unpack why this happens, what puts you at risk, and what you can actually do today to protect your sightno jargon, just friendly, straightforward advice.
What Is NTG
NTG falls under the umbrella of openangle glaucoma, but the key difference is the intraocular pressure (IOP). While most glaucoma patients have IOP readings >21mmHg, NTG patients typically sit comfortably below that thresholdoften 1021mmHg. Yet their optic nerves still show the classic signs of damage: thinning of the retinal nerve fiber layer and loss of peripheral vision.
The condition accounts for roughly 3040% of glaucoma cases in Asia and about 2025% in Western populations, according to epidemiological surveys from . Its more common in older adults, people of East Asian descent, and those with a thin cornea.
Why It Matters
Understanding the pathophysiology (that fancy word for how it works) matters because it tells us why the usual pressurelowering drops sometimes feel like pouring water into a leaky bucket. If we only chase the IOP number, we might miss the underlying culprits that continue to munch away at the optic nerve.
Grasping the mechanisms also empowers you to ask the right questions at your next eyedoctor visit: Are we looking at my bloodflow health? or Should we consider a neuroprotective supplement? Its the difference between treating a symptom and tackling the root cause.
Core Mechanisms
Vascular Dysregulation
One of the leading theories says that NTG is a vascular disease of the eye. In people with NTG, the tiny blood vessels that feed the optic nerve may spasm, constrict, or simply fail to deliver enough oxygen. This ischemic injury can happen even when the pressure is normal.
Research published in shows that patients with nocturnal bloodpressure dipsa common pattern for people who sleep on their backstend to have faster visualfield loss. Think of it like a garden that gets watered irregularly: the plants (your optic nerve fibers) wilt not because of too much sun (pressure) but because theyre not getting a steady drip.
Mechanical Stress at Normal IOP
Even normal pressure can be too much for some eyes. The lamina cribrosaa delicate, sievelike structure where optic nerve fibers exit the eyevaries in thickness and strength among individuals. If yours is thinner or more compliant, the same IOP can produce greater strain, crushing delicate nerve fibers.
A 2022 study in used highresolution OCT imaging to demonstrate that NTG eyes often have a thinner, more posteriorly displaced lamina cribrosa compared with highpressure glaucoma eyes.
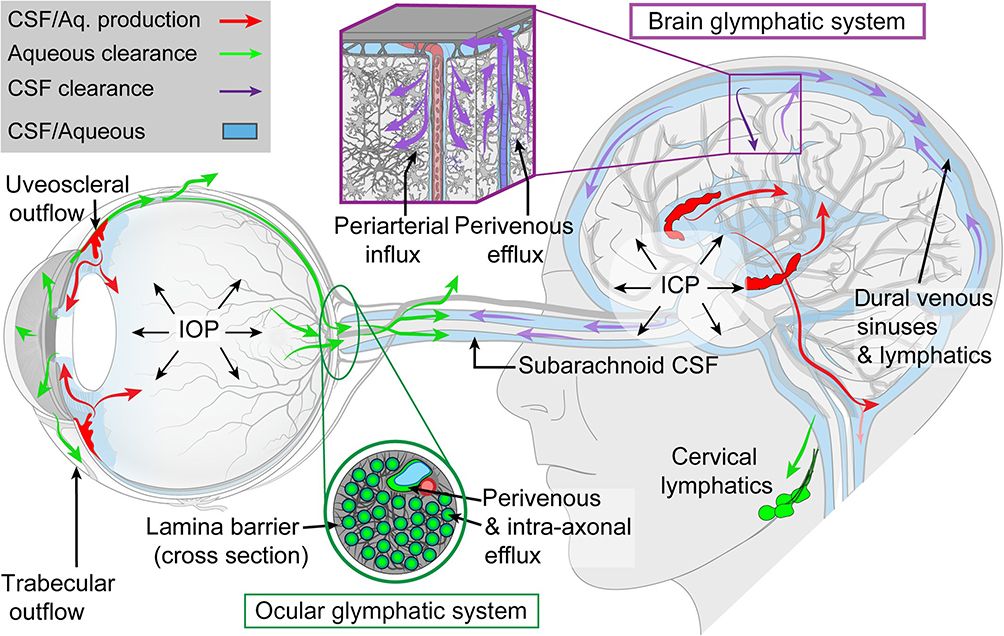
Cerebrospinal Fluid (CSF) and the Glymphatic System
The space around the optic nerve is filled with cerebrospinal fluid. When CSF pressure is low relative to IOP, a pressure gradient forms that can pull the lamina cribrosa outward, again stressing the nerve fibers. Some scientists call NTG a glymphopathy because impaired CSF flow may hinder waste clearance, letting toxic metabolites accumulate.
Evidence from a 2021 review in supports this link, noting that patients with low CSF pressure often present with NTG.
Genetic & Molecular Factors
Genes arent destiny, but they can tilt the odds. Mutations in the OPTN and TBK1 genes have been associated with NTG, especially in families where the disease appears at a young age. These genes meddle with mitochondrial function and the cells stress response, making opticnerve cells more vulnerable.
The 2018 highlighted how mitochondrial DNA damage could amplify vascular insufficiency, creating a doublewhammy effect.
Inflammation & AutoImmunity (Emerging)
Lowgrade inflammationthink of a smoldering candle rather than a roaring firemight also play a role. Elevated cytokines and microglial activation have been seen in NTG eyes, opening the door to potential neuroprotective treatments in the future.
Clinical Implications
How Fast Does NTG Progress?
On average, NTG progresses at about 0.51dB loss per year on standard visualfield tests. However, factors like nocturnal hypotension, sleep apnea, or a history of migraines can speed things up. The key is regular monitoringannual Humphrey visualfield tests and OCT scans can catch subtle changes before they become noticeable in daily life.
Will I Go Blind From NTG?
Complete blindness is rare. Most people retain functional vision for decades if the disease is caught early and managed holistically. The risk of severe vision loss rises sharply when the disease goes untreated for many years, especially if vascular risk factors arent addressed.
Is NTG Hereditary?
Family history does increase riskstudies suggest a 23 higher chance if a close relative has NTG. Specific genetic variants, like the aforementioned OPTN, are found more often in hereditary cases, but lifestyle and systemic health still heavily influence outcomes.
Why Is NTG Harder to Treat?
Because the problem isnt just pressure. Conventional eyedrop regimens that lower IOP (like prostaglandin analogues) often only modestly slow progression. The harder to treat label reflects the need for a multipronged approach: vascular health, neuroprotection, and sometimes surgery.
RiskFactor Checklist
| Risk Factor | Why It Matters |
|---|---|
| Low systemic blood pressure (especially at night) | Reduces opticnerve perfusion |
| Migraine or Raynauds phenomenon | Indicative of vascular dysregulation |
| Thin corneas | May signal a structurally weaker eye |
| Myopia (nearsightedness) | Alters opticnerve anatomy |
| Sleep apnea | Causes intermittent oxygen dips |
| Family history of NTG | Genetic predisposition |
Diagnosis & Monitoring
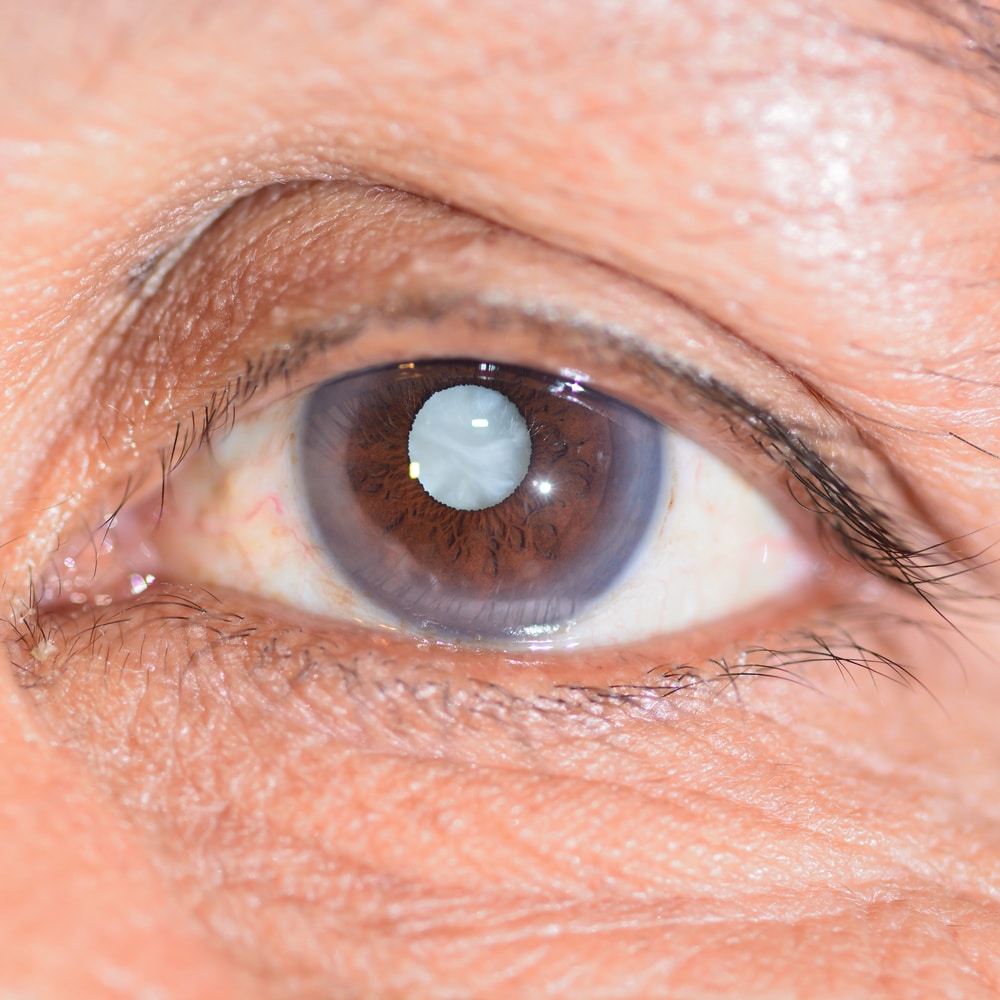
Typical Symptoms
NTG usually sneaks up quietly. Early signs include:
- Gradual loss of peripheral (side) visionlike watching a movie in a theater where the edges darken.
- Difficulty seeing in lowlight conditions.
- Occasional eye strain or floaters that mask underlying damage.
Because the pressure is normal, many patients are surprised when an eye exam uncovers the issue.
Tools We Trust
Optical Coherence Tomography (OCT) provides highresolution images of the retinal nerve fiber layer (RNFL) and ganglioncell complex, letting doctors spot thinning before you notice any vision change.
Visualfield testing (Humphrey) maps the functional loss across your field of view. Repeating this test yearly creates a progression graph that can reveal even tiny declines.
Newer Optical Coherence Tomography Angiography (OCTA) can visualize bloodflow deficits in the opticnerve head, directly tying into the vascular theory.
NTG vs. OpenAngle Glaucoma
| Feature | NormalTension Glaucoma | OpenAngle Glaucoma (HighPressure) |
|---|---|---|
| IOP Range | 21mmHg (often 1218) | >21mmHg |
| Primary Damage Mechanism | Vascular insufficiency, lamina cribrosa susceptibility | Mechanical stress from elevated pressure |
| Typical Progression Speed | 0.51dB/year (variable) | 12dB/year (generally faster) |
| Response to IOPLowering Drops | Modest benefit | Significant benefit |
| Risk Factors | Low BP, migraines, sleep apnea, thin corneas | Age, high myopia, African ancestry |
Management & Treatment Options
PressureLowering Still Helps
Even though the pressure is normal, most specialists still aim for a 2030% reduction. Prostaglandin analogues (like latanoprost) are usually firstline because theyre effective and oncedaily. For some, laser trabeculoplasty can give an extra pressure dip without the hassle of drops.
Addressing Vascular Health
If your bloodpressure dips at night, talk to your primary doctor about adjusting antihypertensive timing or medication type. Some clinicians prescribe lowdose calciumchannel blockers to improve ocular blood flow.
Screening for sleep apnea (overnight pulseox testing) can be a gamechanger. Treating apnea with CPAP often stabilizes nocturnal oxygen levels and, anecdotally, slows visualfield loss.
NeuroProtective Strategies
Medications like brimonidine have shown modest neuroprotective properties beyond pressure reduction. Oral supplementsciticoline, omega3 fatty acids, and coenzymeQ10are popular adjuncts, though you should discuss them with your eyecare provider first.
Lifestyle Tweaks
- Keep a consistent sleep schedule; avoid going to bed on an empty stomach.
- Stay hydrateddehydration can momentarily lower blood pressure.
- Gentle aerobic exercise (e.g., walking) improves overall circulation.
- Limit caffeine spikes if youre prone to bloodpressure fluctuations.
Emerging Therapies
Clinical trials are exploring endothelin1 antagonists and geneediting approaches targeting OPTN. While still experimental, they signal a future where treatment is personalized to your underlying pathophysiology.
RealWorld Stories
Mikes NightTime BloodPressure Dip
Mike, 58, was diagnosed with NTG after a routine visualfield test showed a subtle peripheral defect. His ophthalmologist noted normal IOP but a particularly thin lamina cribrosa. A 24hour BP monitor revealed a 20% drop during sleep. Adjusting his antihypertensive medication and adding lowdose nifedipine stabilized his visual field over the next three years.
Marias Genetic Insight
Maria, 42, has a family history of NTG. She underwent genetic testing, which identified an OPTN mutation. Knowing this, her doctor opted for tighter IOP control (target <12mmHg) and incorporated OCTA monitoring every six months. So far, Marias vision remains stable, and she feels empowered by understanding her why.
What Doctors Say
Treating NTG is like tending a garden, says Dr. Liu, a boardcertified glaucoma specialist. You cant just water the soil (lower pressure); you have to ensure the irrigation system (vascular supply) works and protect the seedlings (nerve cells) from pests (oxidative stress).
Conclusion
Normaltension glaucoma pathophysiology is a mosaic of vascular, mechanical, and genetic pieces. By recognizing that normal pressure doesnt mean no danger, you can work with your eye doctor to craft a comprehensive planone that attacks the pressure, boosts blood flow, shields nerve cells, and embraces lifestyle changes.
If you or someone you love has been diagnosed with NTG, schedule that regular OCT and visualfield check, discuss vascular health with your primary care physician, and dont shy away from asking about neuroprotective options. Knowledge is the best lens through which to keep your world sharp.
Whats your experience with NTG? Have you tried any lifestyle tweaks that helped? Share your story in the commentsyour insights might be the very thing another reader needs.
For related eye conditions that can affect vision and eye comfort, consider reading more about dry eye disease and how it may coexist with other ocular issues.
FAQs
What causes optic nerve damage in normal-tension glaucoma?
Optic nerve damage in normal-tension glaucoma (NTG) mainly arises from a combination of vascular dysregulation, mechanical strain on a structurally vulnerable lamina cribrosa, and impaired cerebrospinal fluid circulation, all occurring despite normal intraocular pressure levels.
How does vascular dysregulation contribute to NTG?
In NTG, small blood vessels supplying the optic nerve may spasm or constrict, leading to insufficient oxygen delivery (ischemia). This vascular insufficiency results in optic nerve damage independent of eye pressure.
What role does the lamina cribrosa play in NTG pathophysiology?
The lamina cribrosa is a sieve-like structure where optic nerve fibers exit the eye. In NTG patients, it is often thinner or more compliant, making it more susceptible to strain and damage even under normal eye pressure.
Are genetic factors involved in NTG?
Yes, mutations in genes such as OPTN and TBK1 are linked to NTG. These affect mitochondrial function and cellular stress responses, making optic nerve cells more vulnerable to damage.
Can lowering intraocular pressure help with NTG?
Lowering intraocular pressure by 20-30% is still beneficial in NTG, though the effect is modest compared to high-pressure glaucoma. Managing vascular health and neuroprotection is also essential for treatment.