Bottom line: if you spot a decorticate posturing seizure, the brains upper pathways are under serious stress. The outlook can swing anywhere from hopeful to critical, and the difference hinges on what caused the posturing, how quickly help arrives, and what followup care looks like. Lets walk through what this phenomenon means, why it happens, and what you can do if you ever face it. For families managing complex neurological care, resources on Exondys 51 assistance can sometimes help with medication access and support during recovery.
What Is Decorticate?
Definition & Core Features
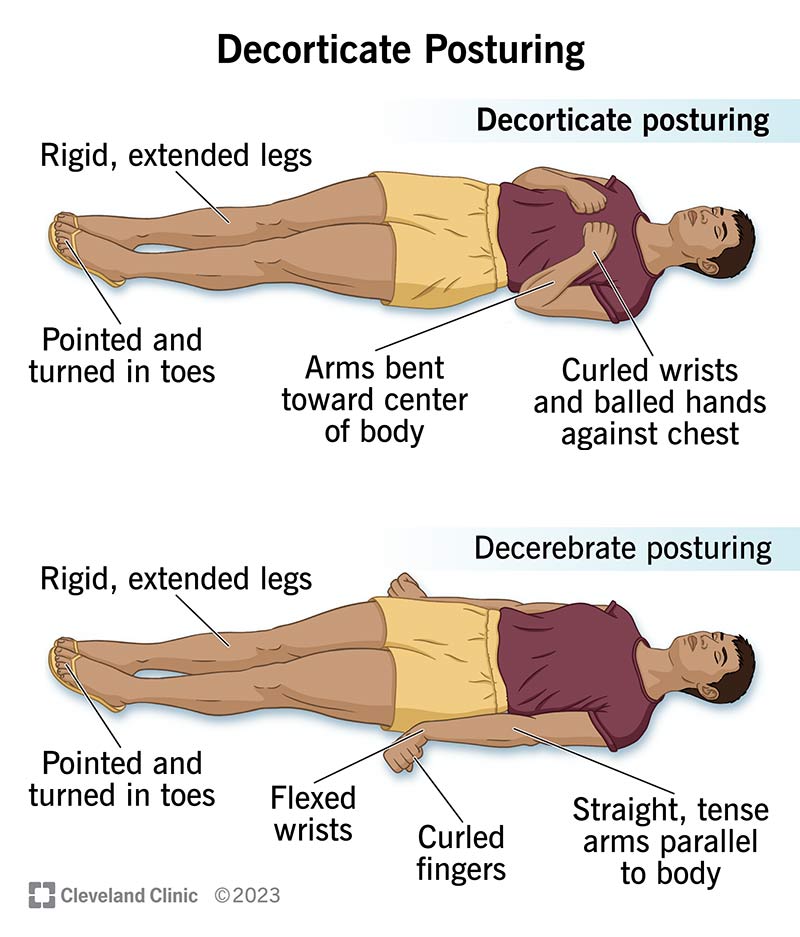
Decorticate posturing is a type of abnormal body posture that typically shows up after a severe brain injury or during a prolonged seizure. The hallmark signs are:
- Flexed elbows and wrists, with the hands clenched into fists.
- Extended, internally rotated legs.
- Increased muscle tone, especially in the upper limbs.
Unlike the rhythmic jerking of a classic tonicclonic seizure, this posture is sustained the limbs stay locked in place until the underlying cause is addressed.
How It Differs From Typical Seizure Activity
Most seizures involve rapid, repetitive movements or a loss of consciousness followed by a brief postictal fatigue. Decorticate posturing, on the other hand, is more about the brains motor pathways being cut off at a higher level, leading to a permanentlooking flexion. Its a neurological alarm bell rather than a seizures dance routine.
Visual Cue Checklist
If you ever need a quick visual guide, remember the flexandextend rule: arms flexed, legs extended. Spotting this combination should immediately prompt emergency action.
Why It Happens
NeuroAnatomical Pathway
The posture originates when the corticospinal tract the highway that sends voluntary movement signals from the brains cortex down to the spinal cord is damaged above the red nucleus in the midbrain. When that upper route is compromised, the brain defaults to older, more primitive reflex pathways, producing the characteristic flexedarm pose.
Common Triggers
Several scenarios can unleash a decorticate posturing seizure:
- Severe traumatic brain injury (TBI) a blow that bruises or bleeds the brain.
- Massive intracranial hemorrhage a sudden bleed that raises pressure inside the skull.
- Status epilepticus a seizure that wont stop on its own, overwhelming the brain.
- Large ischemic stroke affecting the cortex or thalamus.
- Brain tumor compressing critical pathways.
RealWorld Case Vignette
Consider 34yearold Alex, a motorcyclist who crashed on a rainy road. He suffered a severe TBI and, after a prolonged seizure, his emergency team noted a decorticate posture. Rapid intubation, seizure control with benzodiazepines, and an emergent CT scan revealed a subdural hematoma pressing on the right hemisphere. Surgical evacuation saved his life, and intensive rehab later helped him walk again.
Comparison with Decerebrate Posturing
| Feature | Decorticate | Decerebrate |
|---|---|---|
| Arm Position | Flexed elbows, clasped fists | Extended, straight arms |
| Leg Position | Extended, internal rotation | Extended, no rotation |
| Brainstem level | Above red nucleus (midbrain) | Below red nucleus (pons/medulla) |
| Typical Prognosis | Variable; often better than decerebrate | Generally poorer |
Decorticate vs Decerebrate
Clinical Distinctions
Both postures signal serious brain injury, but the exact position tells clinicians where the damage lies. Decorticate indicates higherlevel (cortical) injury, while decerebrate points to deeper brainstem involvement. That distinction matters because deeper injuries tend to affect vital functions like breathing and heart rate.
Prognostic Data
Studies show that patients presenting with decerebrate posturing have a higher mortality rateoften quoted between 7090%whereas decorticate posturing survival rates hover around 4060% depending on cause and treatment speed. notes that early aggressive care can shift odds dramatically.
Comparison Chart
| Aspect | Decorticate | Decerebrate |
|---|---|---|
| Severity Indicator | Severe cortical injury | Severe brainstem injury |
| Typical Survival Rate | 4060% | 1030% |
| Common Causes | TBI, large stroke, status epilepticus | Massive bleed, brain herniation |
| Urgency of Intervention | High | Critical, often emergent surgery |
Brain Damage Insights
Affected Regions
Decorticate posturing tells us the damage likely involves the cerebral hemispheres, thalamus, or internal capsuleareas that funnel signals from the cortex to the spinal cord. When the pathways to the red nucleus are cut, the body reverts to the older flexor reflex.
Typical Etiologies
The biggest culprits behind decorticate posturing damage to what part of brain are:
- Diffuse axonal injury from highspeed trauma.
- Large hemorrhagic strokes that compress the cortical white matter.
- Severe cerebral edema secondary to infection or metabolic dysfunction.
- Spaceoccupying tumors that press on the internal capsule.
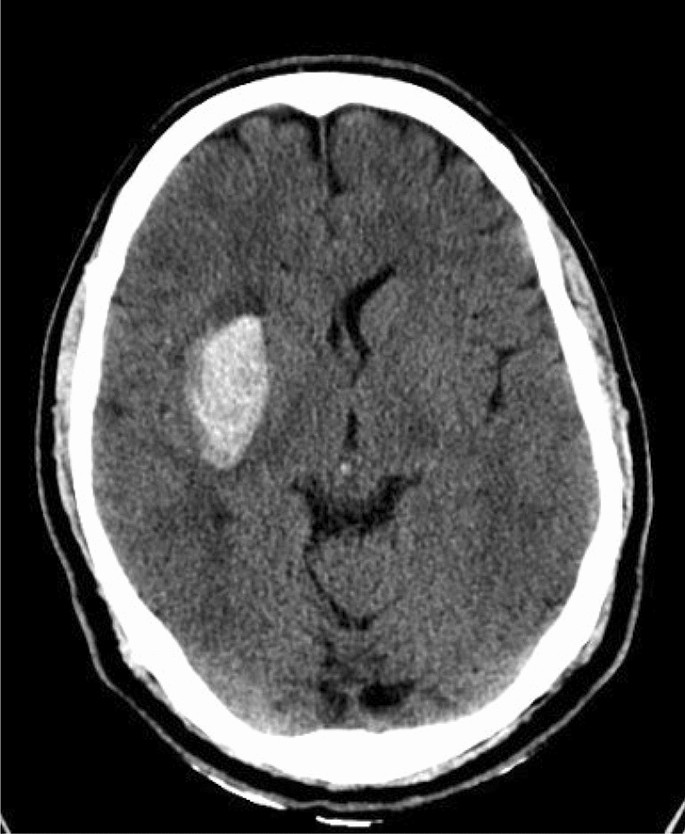
Imaging Pearls
On a CT scan, look for hyperdense areas in the basal ganglia or signs of midline shift; MRI will show more subtle whitematter disruption. Radiologists often flag a hunchedposture sign when they see lesions above the red nucleus.
Expert Quote
When you see a decorticate pose, think of it as the brains SOS. It tells us the higher motor pathways are offline, and immediate neurocritical care is mandatory, explains Dr. Maria Lopez, a neurointensivist at a leading academic hospital.
Survival & Prognosis
Overall Statistics
According to a metaanalysis published in Neurocritical Care, the decorticate posturing survival rate across all etiologies sits at roughly 55% when managed in a specialized ICU. The numbers rise to 70% for younger patients with isolated TBI and drop below 30% for older individuals with multisystem trauma.
Factors That Improve Odds
Speed is everything. The sooner you stop the seizure, control intracranial pressure, and begin targeted neuroprotective therapies, the better the chances of recovery. Other favorable factors include:
- Age under 45.
- Absence of significant comorbidities (e.g., heart disease).
- Prompt surgical evacuation of hematomas when indicated.
- Early initiation of rehabilitation.
Rehabilitation Pathways
Even after the acute crisis, survivors often need intensive PT/OT, speech therapy, and cognitive rehab. A structured program can help rewire some of the lost pathways, especially when the injury is higherlevel rather than deep brainstem.
Patient Story
Jenna, a 28yearold teacher, suffered a seizure on the way to work that spiraled into decorticate posturing due to a hidden arteriovenous malformation. After emergent embolization and weeks in the ICU, she now attends weekly physio and gradually regains fine motor control. I thought Id never write again, she says, but with the right team, Im back to grading papers.
Emergency Management Steps
ABCs & Seizure Stop
The first priority is the classic ABCs Airway, Breathing, Circulation. Secure the airway (often via intubation), give 100% oxygen, and control blood pressure. Then, halt the seizure with a rapidacting benzodiazepine like lorazepam or midazolam.
Pharmacologic Arsenal
Beyond benzodiazepines, clinicians may add:
- Loading doses of levetiracetam or fosphenytoin for ongoing seizure control.
- Hypertonic saline or mannitol if intracranial pressure spikes.
- Propofol infusion for refractory status epilepticus.
Monitoring Strategies
Continuous EEG monitoring is essential to detect nonconvulsive seizures that can keep the brain under stress. Intracranial pressure (ICP) monitors, repeat CT scans, and serial neurological exams guide treatment adjustments.
Guideline References
The article on decorticate posturing outlines the same stepwise approach, underscoring the need for rapid neurocritical care.
When Neurosurgery Is Considered
If imaging shows a surgically accessible hematoma, significant edema, or herniation risk, neurosurgeons may perform:
- Decompressive craniectomy.
- Hematoma evacuation.
- External ventricular drain placement for CSF diversion.
Frequently Asked Questions
What does decorticate posturing indicate?
It signals severe injury to the brains upper motor pathways, often above the red nucleus, and requires immediate medical attention.
Is decorticate posturing always a sign of death?
No. While its a grave sign, many patients survive, especially when treatment is swift and the underlying cause is reversible.
Can medication cause a decorticatelike posture?
Certain neurotoxic drugs can mimic the posture, but true decorticate posturing is almost always linked to structural brain injury.
How is decorticate different from decerebrate posturing?
Decorticate involves flexed arms and extended legs (higherlevel injury); decerebrate shows straight arms and legs (lowerbrainstem injury). The latter generally has a worse prognosis.
What is the prognosis for decorticate posturing after a seizure?
Survival rates range from 4060% overall, improving with younger age, rapid seizure control, and aggressive neurocritical care.
Which is worse, decorticate vs decerebrate posturing?
Decerebrate is typically considered worse because it reflects deeper brainstem damage, which compromises vital functions more severely.
What causes decorticate vs decerebrate posturing?
Both arise from brain injury, but decorticate stems from damage above the red nucleus (cortex, internal capsule), while decerebrate stems from damage below it (pons, medulla).
Understanding these nuances can make the difference between panic and preparedness. If you ever encounter a decorticate posturing seizure, remember the steps: call emergency services, stay calm, protect the persons airway, and act fast. Knowledge empowers you to be a better ally in a crisis.
Stay informed, stay compassionate, and dont hesitate to reach out to a medical professional if you have any lingering questions. Your vigilance could be the lifeline someone needs.
FAQs
What does decorticate posturing seizure indicate?
It indicates serious injury to the brain’s upper motor pathways, often above the midbrain’s red nucleus, requiring immediate medical attention.
Is decorticate posturing seizure always fatal?
No. While it signals severe brain stress, many patients survive with rapid, appropriate emergency care and treatment of the underlying cause.
How can decorticate posturing be differentiated from typical seizure movements?
Decorticate posturing is a sustained abnormal flexion posture (arms bent, legs extended), unlike most seizures that involve rhythmic jerking or convulsions.
What are the common causes of decorticate posturing seizures?
They include severe traumatic brain injury, massive intracranial hemorrhage, status epilepticus, large strokes, and brain tumors compressing motor pathways.
What emergency steps should be taken if someone shows decorticate posturing during a seizure?
Immediately call emergency services, secure the airway, provide oxygen, stop the seizure with rapid-acting benzodiazepines, and get urgent neuroimaging and critical care.