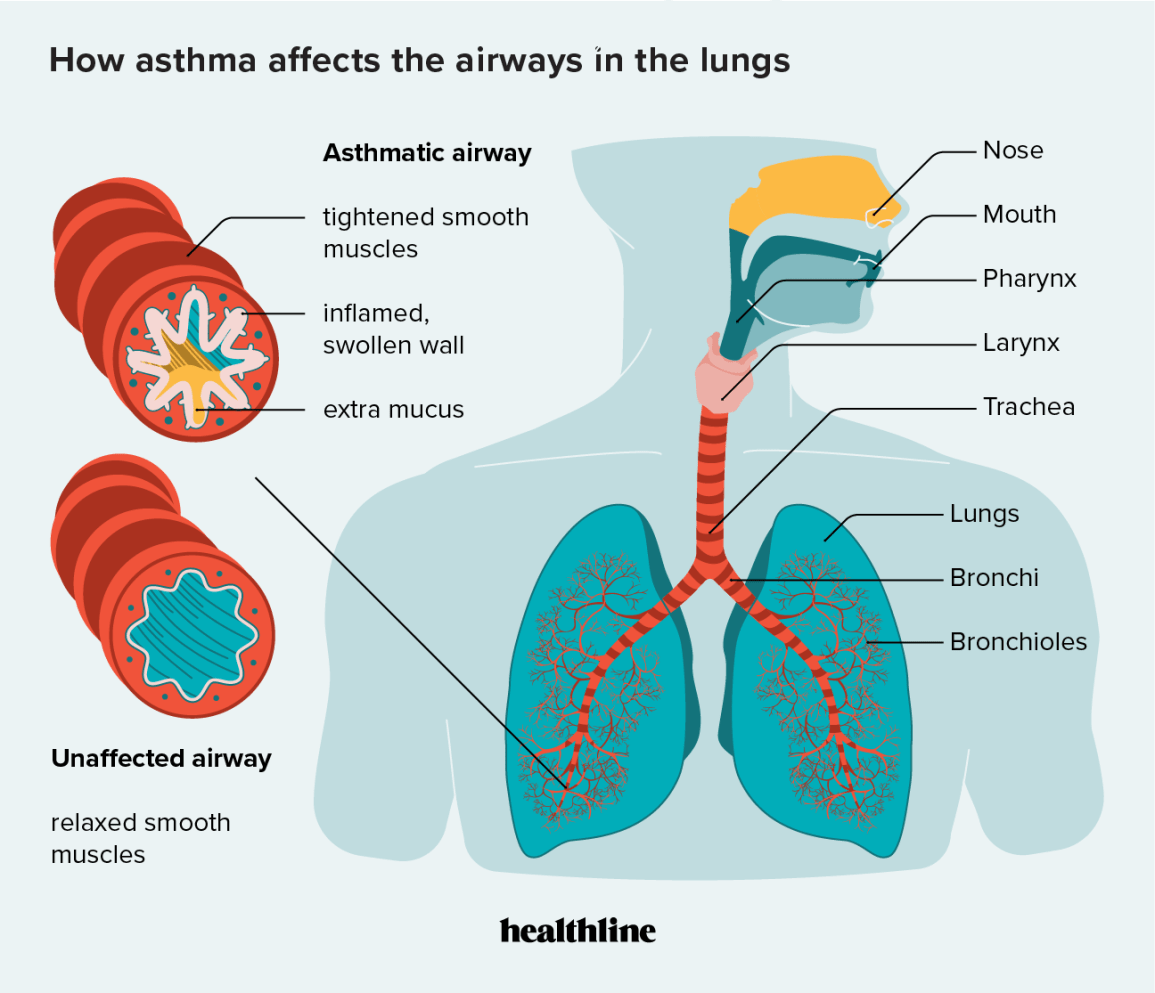
When you have asthma, the walls of your airways become inflamed, swollen, and may produce extra mucusthose are the asthma lung changes that can tighten breathing and trigger attacks. Understanding these structural shifts helps you spot early warning signs, avoid long-term scarring, and decide when you need professional help.
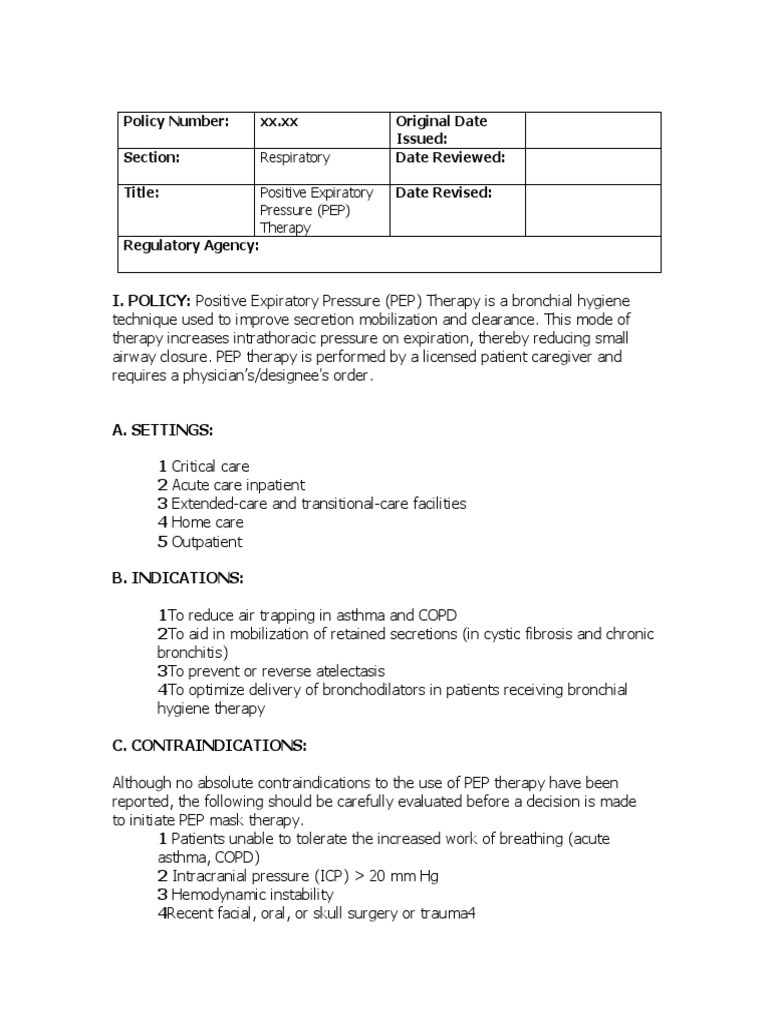
Think of your airway like a garden hose that gradually gets clogged with mineral deposits. If you don't clean it out early, the flow gets weaker and the hose may even crack. The same principle applies to your lungs, and the good news is that many of these changes are preventable or reversible with the right care. In chronic lung diseases such as cystic fibrosis, maintaining open and clear airways is even more complex, and special strategies like cystic fibrosis airway clearance or other airway clearance methods are crucial routine treatments for affected individuals.
How Asthma Alters Lungs
What exactly are the structural changes in asthma-affected lungs?
Inflammation, smooth muscle growth, and mucus overload
Asthma triggers an inflammation cascade that thickens the bronchial walls. Tiny muscles around each airway start to hypertrophy (grow bigger), making the passageway tighter. At the same time, mucus gland hyperplasia creates sticky secretions that further block airflow. Collectively, doctors call this process airway remodeling.
According to a review in StatPearls, these changes can start as early as childhood and accelerate with repeated severe attacks.
Why do these changes narrow the airway?
Physics of airflow and cytokine activity
Air moves through a pipe. If the pipe's radius shrinks just a little, resistance jumps dramatically (think of a garden hose you tried to squeeze). Inflammation releases cytokines like IL4, IL5, and IL13, which signal the muscles to tighten and the lining to swell. The result? A narrower path for air and a louder wheeze.
Can asthma lung changes become permanent?
Reversible vs. irreversible remodeling
Early-stage changes are often reversible with inhaled corticosteroids (ICS) and good trigger control. However, if the inflammation persists for years, fibrosis (scar tissue) can set in, making some narrowing permanent. A long-term study in Chest found that patients who delayed regular controller therapy were twice as likely to develop fixed airway obstruction.
How are lung changes visualized?
Imaging and functional tests
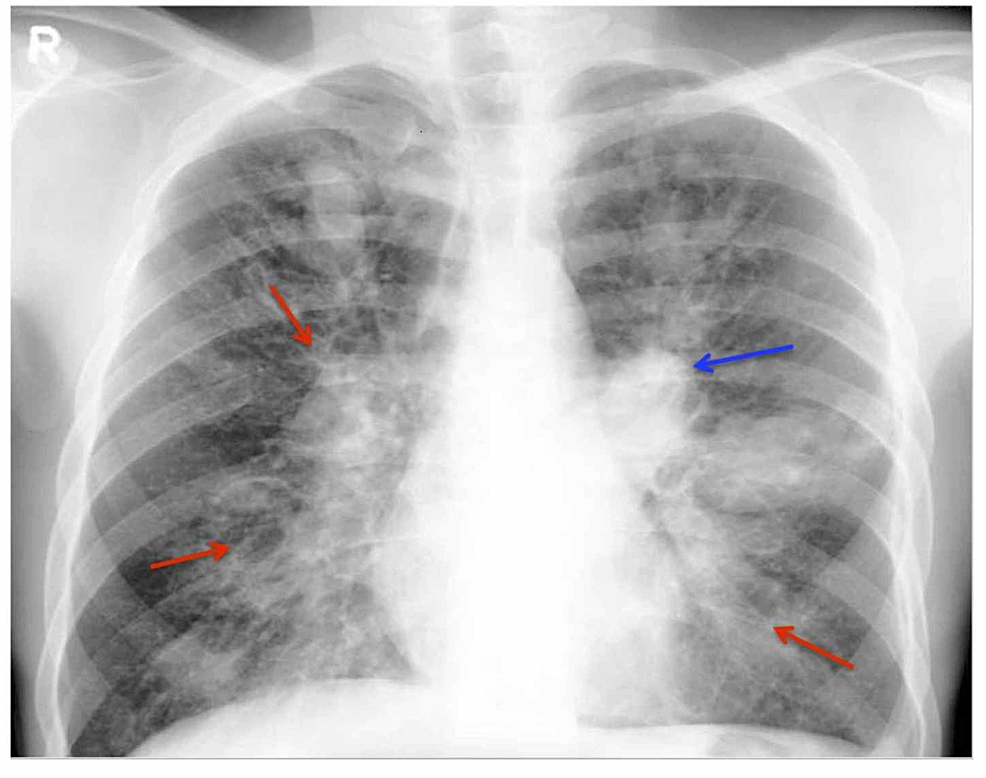
- Chest X-ray: May show hazy areas but is not sensitive for early remodeling.
- High-resolution CT: Shows airway wall thickness and early fibrosis.
- Spirometry: A drop in FEV (forced expiratory volume) after a bronchodilator suggests irreversible changes.
- Peak flow monitoring: Helps you notice day-to-day variations that could signal worsening remodeling.
Symptoms That Signal Changes
What symptoms indicate early airway remodeling?
Persistent tightness, chronic cough, reduced stamina
If you find that a quick puff of your reliever no longer eases that tight-chest feeling, or you're coughing more at night even after your asthma seems under control, these could be the first clues of structural change. Many people describe it as "my lungs feel heavier even when they're at rest."
How do asthma lung scarring symptoms differ from regular attacks?
Dry cough, subtle shortness of breath, occasional crackles
Typical asthma spikes involve wheezing, rapid onset, and quick relief with a rescue inhaler. Scarring, on the other hand, may present as a dry, nonproductive cough that lingers, mild shortness of breath on minimal exertion, and sometimes a faint Velcro crackle heard by a clinician.
When should I worry that asthma could be life-threatening?
Red-flag signs and emergency steps
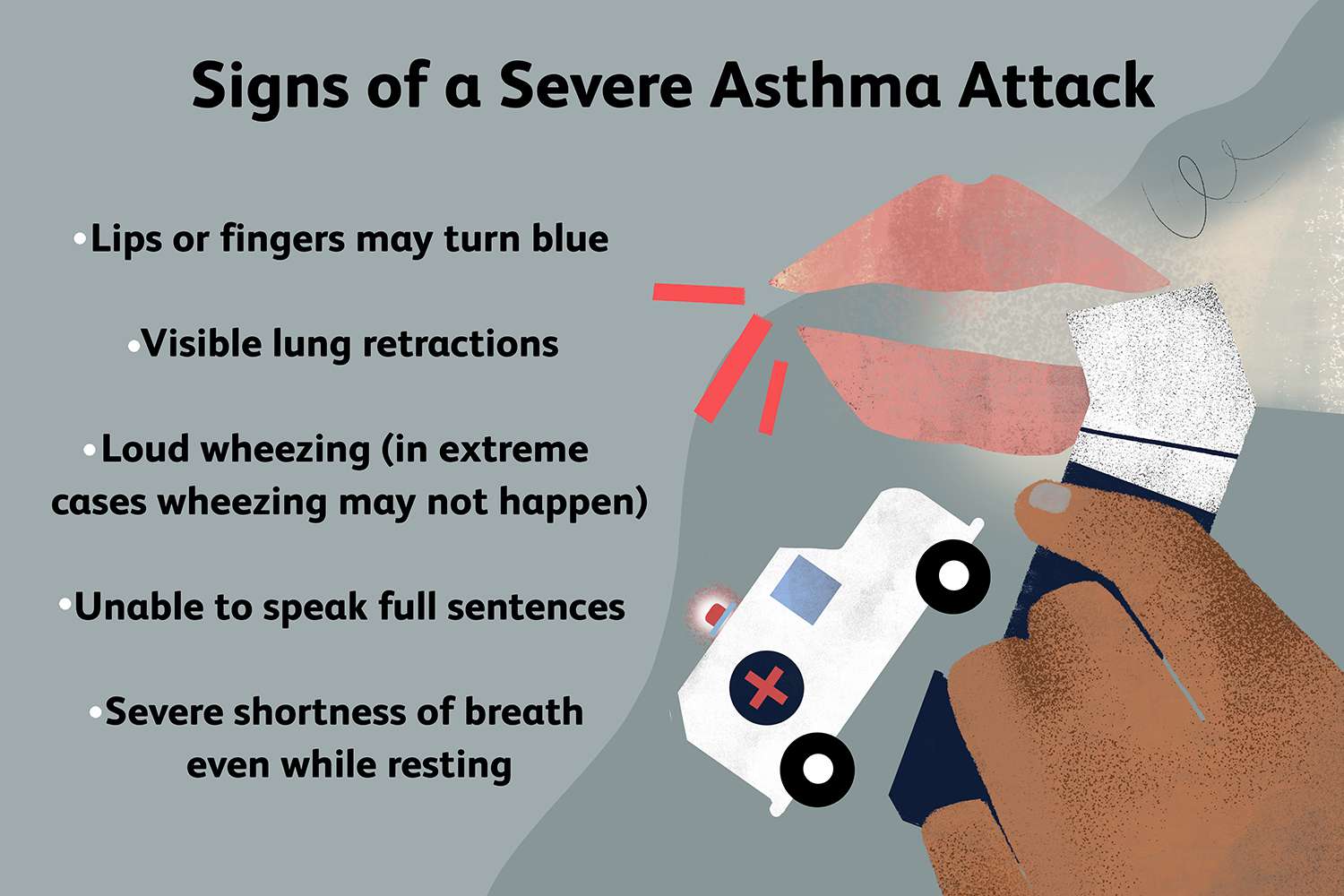
The question can asthma kill you? is scary, but the reality is that status asthmaticusa severe, unrelenting attackcan be fatal if oxygen drops below 90% and help isn't received quickly. Look out for:
- Rapid breathing that doesn't improve with your rescue inhaler
- Chest tightness that feels like a vice grip
- Blue-tinged lips or fingertips
- Confusion or inability to speak full sentences
If any of these appear, call emergency services immediately and use your prescribed oral steroids if you have them.
Do other conditions mimic these changes?
Overlap with COPD, bronchiectasis, and ABPA
Chronic obstructive pulmonary disease (COPD) and certain infections can produce similar airway thickening. A careful medical history and targeted tests (like sputum analysis for allergic bronchopulmonary aspergillosis) help differentiate them. It's notable that people with other chronic lung conditionsnotably cystic fibrosisoften face even stricter requirements for infection control and cf social distance to protect themselves and others from cross-infection risks.
Causes & Risk Factors
What are the main triggers that accelerate lung changes?
Repeated attacks, allergens, smoke, infections
Every severe flare you experience adds a brick to the remodeling wall. Key accelerators include:
- Frequent severe attacks (more than two a month)
- Allergen exposuredust mites, pet dander, pollen
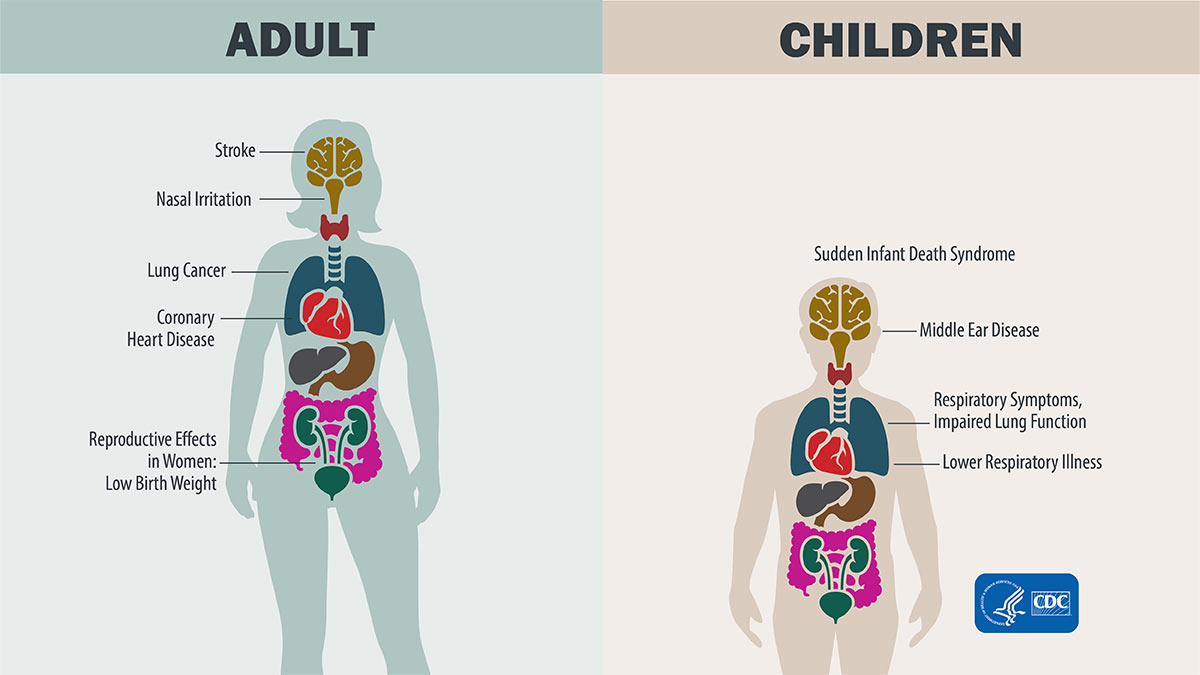
- Tobacco smoke, indoor pollutants, chemical fumes
- Viral respiratory infections, especially RSV and influenza
What are the 5 biggest underlying causes of asthma?
Genetics, atopy, occupation, obesity, infections
| Cause | How it contributes |
|---|---|
| Genetic predisposition | Family history of atopy or asthma raises baseline risk. |
| Allergic (atopic) inflammation | IgE-mediated response to common allergens triggers chronic airway irritation. |
| Occupational irritants | Exposure to chemicals like isocyanates can cause occupational asthma. |
| Obesity & metabolic syndrome | Leptin and systemic inflammation worsen airway hyperresponsiveness. |
| Early-life respiratory infections | Severe RSV or rhinovirus infections can alter lung development. |
Which types of asthma are most prone to lung remodeling?
Severe persistent, late-onset, nonallergic
Clinicians group asthma into extrinsic (allergic) and intrinsic (nonallergic) forms. The severe-persistent and late-onset types often show the fastest progression toward airway wall thickening because they tend to be undertreated or misdiagnosed.
How do lifestyle factors influence risk?
Activity, diet, stress, and sleep
Regular aerobic exercise helps clear mucus and improves lung capacity. A diet rich in omega-3 fatty acids and antioxidants can dampen inflammatory pathways. Chronic stress raises cortisol, which paradoxically worsens inflammation in some people. Even sleep quality matterspoor sleep can heighten airway sensitivity.
Is there a link between asthma and COPD?
Asthma-COPD overlap (ACO)
People who smoke heavily and have a longstanding asthma diagnosis may develop ACO, a blend of both diseases that accelerates remodeling. The World Health Organization notes that ACO patients have higher hospitalization rates and faster lung-function decline.
Diagnosis: Spotting Early Changes
What tests reveal airway remodeling?
Spirometry, plethysmography, CT, biomarkers
Standard spirometry shows how much air you can push out in one second (FEV). If the post-bronchodilator increase is less than 12% of the baseline, it suggests some fixed obstruction. Body plethysmography measures airway resistance directly, while high-resolution CT can visualize wall thickening. Biomarkers like FeNO (fractional exhaled nitric oxide) and sputum eosinophils give clues about the underlying inflammation.
When should a doctor order imaging?
Unexplained declines, suspicion of fibrosis
If you notice a steady drop in peak flow over weeks, or your doctor hears crackles during an exam, a CT scan may be recommended to rule out early fibrosis. Imaging isn't required for every asthma patient, but it's a powerful tool when you suspect permanent changes.
Can a primary-care doctor diagnose asthma lung changes?
Referral to specialists when needed
Yes, your family doctor can run spirometry and assess symptom patterns. However, definitive confirmation of remodeling often needs a pulmonologist's expertiseespecially if you're a candidate for biologic therapy or have an atypical presentation.
Treatment & Prevention
How do inhaled corticosteroids (ICS) stop remodeling?
Anti-inflammatory action and evidence
ICS target the inflammatory cascade at its source, reducing cytokine production and limiting smooth muscle growth. A randomized trial published in The Lancet showed that consistent high-dose fluticasone reduced airway wall thickness by up to 20% after two years of therapy. The key is daily adherencenot just using them during flareups.
Do biologics reverse existing lung changes?
Anti-IL5, anti-IL4R and clinical outcomes
Biologics such as mepolizumab (anti-IL5) and dupilumab (anti-IL4R) have demonstrated reductions in eosinophilic inflammation and modest improvements in CT-measured wall thickness. They're especially helpful for patients with severe eosinophilic asthma who still experience attacks despite high-dose ICS.
According to , dupilumab lowered the rate of severe exacerbations by 50% and slowed the progression of airway remodeling.
What lifestyle actions minimize risk?
Trigger avoidance, exercise, nutrition
- Trigger checklist: Keep windows closed on high pollen days, use HEPA filters, avoid indoor smoking, and control humidity to prevent mold.
- Exercise: Aim for 150 minutes of moderate aerobic activity per weekthink brisk walking, swimming, or cycling.
- Nutrition: Incorporate fatty fish, nuts, berries, and leafy greens for their antioxidant benefits.
- Stress management: Mindfulness, yoga, or simple breathing exercises can lower cortisol spikes that aggravate airway reactivity.
Those with certain conditions, like cystic fibrosis, may require additional precautions and adapted daily routines; expert cf relationship advice can help patients and families manage the social and lifestyle complexities associated with long-term disease management.
When is lung-function monitoring essential?
Regular testing and home tools
For moderate-to-severe asthma, schedule spirometry every six months. At home, a peak flow meter helps you catch early declines; a drop of 20% from your personal best should trigger a medication review.
Can severe asthma lead to fatal outcomes?
Understanding the risk and emergency plan
While most asthma deaths occur in people who underestimate their severity, having a clear action plan reduces that risk dramatically. Keep a written emergency plan, ensure you have a rescue inhaler plus a short course of oral steroids on hand, and educate family members on when to call emergency services.
Real-World Patient Stories
A case where early treatment prevented scarring
Young adult's journey
Emily, a 27-year-old graphic designer, experienced two severe attacks in her first decade of asthma. After her pulmonologist prescribed daily low-dose fluticasone and a personalized trigger-avoidance plan, her FEV stayed steady over five years. She says, "I realized that using my inhaler every day, even when I felt fine, was the secret sauce."
When delayed care led to permanent changes
Middle-age man's lesson
Mark, 42, ignored his worsening cough for years, thinking "it's just a cold." By the time he finally sought help, a high-resolution CT showed noticeable airway wall thickening and early fibrosis. He now follows a strict medication schedule and attends regular follow-ups, noting, "I wish I'd listened earlier."
Tips from asthma-living patients
Everyday hacks to stay on track
- Set a phone alarm labeled "Asthma Check" to remind you to use your controller inhaler.
- Keep a spare inhaler in your car, work bag, and at the office.
- Pair medication time with a daily habitlike brushing teethto build routine.
- Log symptoms in a notebook; patterns often emerge that you can discuss with your doctor.
Quick-Fire Q&A Section
Can asthma cause lung scarring?
Yes; chronic inflammation can lead to airway remodeling and, in severe cases, fibrosis (scar tissue).
Is asthma fatal?
Rarely, but an uncontrolled severe attack (status asthmaticus) can be life-threatening if not treated promptly.
How many types of asthma are there?
Clinically, we talk about allergic (extrinsic) and nonallergic (intrinsic) asthma, plus categories based on severity: intermittent, mild-persistent, moderate-persistent, and severe-persistent.
What are the top 5 asthma causes?
Genetics, allergic inflammation, occupational irritants, obesity, and early-life respiratory infections.
What are common asthma symptoms?
Wheezing, shortness of breath, chest tightness, and coughespecially at night or early morning.
Conclusion
Asthma isn't just an occasional wheeze; it can reshape the very architecture of your lungs. By spotting the subtle signs of asthma lung changes, staying on top of medication, and making smart lifestyle choices, you can haltor even reversemany of those changes. Remember, your lungs are resilient, but they need a consistent partner in care.
If you've noticed any of the symptoms we discussed, or if you have questions about your inhaler routine, don't hesitate to reach out to your healthcare provider. Share your own story in the comments belowyour experience might be the spark that helps someone else take that crucial next step toward healthier lungs.
FAQs
What are the main structural changes in asthma‑affected lungs?
Asthma causes airway inflammation, smooth‑muscle hypertrophy, and mucus‑gland hyperplasia, collectively known as airway remodeling.
Can asthma lung changes become permanent?
Early changes are often reversible with proper controller therapy, but prolonged inflammation can lead to fibrosis and fixed airway obstruction.
How do I know if my asthma is causing airway remodeling?
A noticeable drop in peak flow, reduced response to rescue inhalers, or a persistent cough at night may indicate early remodeling.
What tests can detect airway remodeling?
Spirometry, body‑plethysmography, high‑resolution CT scans, and biomarkers such as FeNO or sputum eosinophils help identify structural changes.
Do biologic medications reverse existing lung changes?
Biologics like mepolizumab and dupilumab reduce eosinophilic inflammation and can modestly improve airway wall thickness, slowing further remodeling.