Core Reason Explained
What does nocontrast actually mean?
In imaging, contrast refers to an iodinebased dye that makes blood vessels glow on a CT scan. When we say nocontrast CT, we simply mean the scan is taken without injecting that dye. The images are just the natural density differences of brain tissue and blood.
Hemorrhagic vs. Ischemic Stroke why the distinction matters
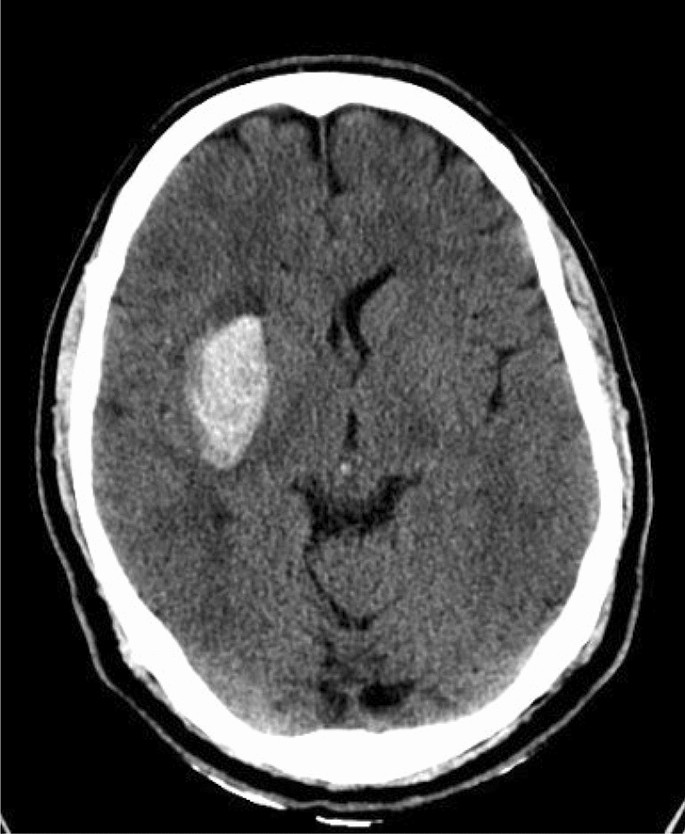
A hemorrhagic stroke is a burst blood vessel a bright white spot on the scan. An ischemic stroke is a clot that blocks blood flow it shows up as a subtle darkening, often invisible in the first hour. The difference is critical because thrombolytic therapy (tPA) is only safe for ischemic strokes; giving it to a patient with a bleed can be catastrophic.
| Finding | Appearance on NCCT | Implication for Treatment |
|---|---|---|
| Hyperdense area | Bright / white | Intracranial hemorrhage no tPA |
| Loss of graywhite differentiation | Slight dimming | Early ischemia may still qualify for tPA |
| No obvious changes | Normal | CT negative still possible clot, need further imaging |
How fast is the scan?
From the moment the patient is on the table, a noncontrast head CT takes under five minutes. That speed is why the American Heart Associations list NCCT as the initial imaging modality of choice.
Benefits of NCCT First
Speed and accessibility
More than 95% of U.S. emergency departments have a CT scanner ready 24/7. In a rural clinic, the same machine can be moved to a nearby hospital within minutes. That universal availability means youre unlikely to wait for an MRI slot when every second counts.
Patient safety and tolerance
No IV line for dye means zero risk of allergic reactions, no worries about kidney function, and safe use in pregnant patients. Its literally plugandplay the patient just lies down, and the scanner does the work.
Costeffectiveness
A plain CT costs roughly $300$500, while adding contrast or ordering an MRI can push the bill over $1,200. For health systems and patients alike, that savings adds up quickly.
Realworld experience
Take Mrs.L., a 68yearold who suddenly slurred her speech on a Tuesday morning. The ER team performed an NCCT in three minutes. The scan showed a clear bleed, so they skipped tPA and called a neurosurgeon immediately. Today, shes recovering at home, and that splitsecond decision saved her life.
Limitations & Alternatives
Low sensitivity for early ischemia
Early on (first hour), a noncontrast CT can miss up to 30% of small infarcts, according to a 2022 study in SpringerOpen. Thats why clinicians often follow up with more sensitive imaging if the clinical picture suggests a stroke despite a normal CT.
When contrast becomes useful
If the initial scan rules out a bleed but the team suspects a largevessel occlusion (think of a clot in the middle cerebral artery), theyll order a CT angiography (CTA) the same scanner with a quick injection of contrast. CTA maps the vessels, helping decide whether endovascular thrombectomy is possible. For guidance on arranging follow-up support and navigating the costs that can come with advanced therapies, some patients find resources on Exondys 51 assistance helpful when coordinating care and financial assistance programs.
MRI for a deeper look
Magnetic resonance imaging, especially diffusionweighted imaging (DWI), catches ischemic changes within minutes of onset, far better than CT. However, MRIs take longer (1530minutes), arent available everywhere, and cant be used with certain metal implants. So the usual pathway is: NCCT CTA if needed MRI if the picture is still unclear.
Decisionflow diagram
Below is a simple flow you might hear the ER team describe:
- Suspected stroke NCCT
- Bleed seen? Hemorrhagic protocol (neurosurgery, avoid tPA).
- No bleed & 4.5h? Consider tPA; if largevessel suspicion add CTA.
- >4.5h or unclear? MRI with DWI for definitive diagnosis.
CT vs MRI Comparison
Accuracy for the ischemic core
MRI DWI boasts ~95% sensitivity for detecting an infarct in the hyperacute window, while NCCT lags behind at 6070%.
Practical considerations
| Modality | Time to Scan | Availability | Contraindications | Typical Acute Use |
|---|---|---|---|---|
| NCCT | 35min | Most EDs | None | Firstline, ruleout bleed |
| CTAngio (contrast) | +23min | Widely available | Contrast allergy, renal failure | Vessel occlusion, thrombectomy planning |
| MRI (no contrast) | 1530min | Limited to tertiary centers | Metal implants, claustrophobia | Confirm infarct, subacute phases |
| MRI (with gadolinium) | +510min | Same as above | Gadolinium allergy, severe CKD | Tumor, infection, detailed vessel wall |
Quick FAQ
How long will a stroke show up on a CT scan? A hemorrhage appears instantly. Early ischemic changes may be subtle for the first 36hours and become clearer after 1224hours.
Guidelines & Protocols Overview
AHA/ASA 2023 recommendations
The American Heart Association and American Stroke Association (AHA/ASA) state that a noncontrast head CT performed within 20minutes of ED arrival is the preferred initial test for all patients with suspected stroke. The guideline emphasizes speed, safety, and the ability to rule out hemorrhage before any thrombolytic therapy.
European Stroke Organisation (ESO) stance
ESO aligns closely, recommending NCCT first, followed by CTAngio if a largevessel occlusion is suspected. Their focus is on stroke code pathways that keep the doortoneedle time under 60minutes.
Sample institutional stroke code checklist
- Activate stroke alert bring patient to CT suite within 5minutes.
- Perform NCCT interpret for bleed.
- If no bleed and <4.5h onset evaluate for tPA eligibility.
- Order CTA if largevessel occlusion is possible.
- Consider MRI if diagnosis remains uncertain after NCCT/CTA.
Patient Practical Takeaways
What to expect during the scan
Youll lie on a narrow table that slides into a doughnutshaped machine. Its quiet, no needles (unless contrast is later needed), and the whole thing takes about five minutes. Technologists may place a small pillow under your head for comfort, but theres no need to fast or change clothes.
Questions you can ask your care team
- Has the bleed been ruled out?
- Will we need a contrast study after this?
- If tPA is possible, whats the next step?
- Should I expect an MRI later, and why?
Downloadable quickreference
Weve put together a printable that summarizes the typical sequence of scans, what each looks for, and the key decisions doctors make at each stage. Keep it handy for yourself or a loved one.
Conclusion
When seconds matter, a noncontrast CT is the speedcoach of stroke imaging it tells doctors fast whether theres blood in the brain, the single most crucial factor in deciding if clotbusting medication is safe. While it isnt perfect at catching the tiniest early ischemic changes, its nearuniversal availability, low cost, and safety make it the undeniable firstline tool championed by the AHA/ASA and major stroke societies. If the plain scan is negative or if a largevessel clot is suspected, doctors will add contrast or move to MRI to finetune the diagnosis and plan advanced therapies. Knowing why no contrast CT for stroke helps you feel more informed, reduces the anxiety of the unknown, and empowers you to ask the right questions during that critical stroke code moment. We hope this guide lights the path for you or anyone you care about when faced with the urgency of a possible stroke.
FAQs
Why is a noncontrast CT used for stroke?
A noncontrast CT is used for stroke because it quickly rules out bleeding in the brain, which is essential before giving clot-busting drugs.
Can a noncontrast CT miss a stroke?
Yes, a noncontrast CT can miss early ischemic changes, especially in the first few hours after stroke onset.
When is contrast used in stroke imaging?
Contrast is used after a noncontrast CT if doctors suspect a large vessel blockage and need to plan advanced treatments like thrombectomy.
Is a noncontrast CT safe for everyone?
Yes, a noncontrast CT is safe for almost everyone, including pregnant patients and those with kidney problems.
How fast is a noncontrast CT for stroke?
A noncontrast CT for stroke takes less than five minutes, making it the fastest way to check for bleeding in the brain.