Inflammatory arthritis is a broad umbrella that covers several immune-driven joint disorders, while rheumatoid arthritis (RA) is the most common and well-known member of that family. Knowing how they differ and how they both differ from osteoarthritis can save you months of uncertainty, guide you to the right doctor, and help you choose a treatment that actually works.
In the next few minutes, we'll walk through the basics, the diagnosis process, treatment options, and even a few rare types you've probably never heard of. Grab a cup of tea, settle in, and let's demystify this together.
What Is Inflammatory Arthritis
Definition and core mechanism
Think of inflammatory arthritis as a group of conditions where the immune system mistakenly attacks the lining of your joints (the synovium). This causes swelling, pain, and eventually damage if left unchecked. Unlike wear-and-tear arthritis, the inflammation comes from inside your body, not from old age or overuse.
Major categories (quick list)
| Type | Key Feature |
|---|---|
| Rheumatoid arthritis | Symmetric small-joint involvement, often hands and feet |
| Psoriatic arthritis | Skin psoriasis plus joint pain |
| Ankylosing spondylitis | Spine-centric stiffness, bamboo spine on X-ray |
| Reactive arthritis | Joint pain after a bacterial infection |
| Juvenile idiopathic arthritis | Onset before age 16 |
| Behet's disease | Oral ulcers, eye inflammation, plus joint pain |
How it differs from noninflammatory arthritis
Noninflammatory arthritis, most commonly osteoarthritis, is caused by mechanical wear on the cartilage. The pain usually worsens with activity and improves with rest. Inflammatory arthritis, on the other hand, often starts with intense morning stiffness that lasts more than 30 minutes and improves as you move. The systemic nature of the disease can also bring fatigue, low-grade fever, or a rashsymptoms you rarely see with plain-old osteoarthritis.
Rheumatoid Arthritis Overview
Basic facts & prevalence
RA affects about 1% of the population worldwide, striking women about three times more often than men. It usually appears between the ages of 30 and 60, but there's no rulekids and seniors can develop it too.
The four stages of rheumatoid arthritis
Understanding the progression helps you see why early treatment matters:
- Stage 1 Synovitis: Inflammation of the joint lining; swelling but no permanent damage.
- Stage 2 Erosions: Bone begins to erode; X-rays may show tiny pits.
- Stage 3 Deformity: Joint structure changes, making daily tasks harder.
- Stage 4 Functional loss: Severe damage leads to loss of mobility and independence.
Typical symptoms & red-flag signs
Think of these as your body's alarm system: morning stiffness lasting >30 minutes, symmetrical swelling of the wrists or fingers, fatigue that feels off-track, and occasionally a low-grade fever. If you notice any of these persisting for more than a few weeks, it's time to get checked.
Is rheumatoid arthritis an autoimmune disease?
Yes. RA is driven by an autoimmune responseyour immune cells target proteins in the joint lining as if they were invaders. This is why disease-modifying drugs that calm the immune system are the cornerstone of therapy.
Who gets RA? Risk factors
Genetics play a role (the HLA-DRB1 gene is a well-known culprit), but lifestyle matters too. Smoking dramatically increases risk, and women's hormonal changes appear to tip the scale.
Diagnosing Inflammatory Arthritis
Clinical evaluation
First, a rheumatologist will ask about your symptoms, family history, and any triggers. They'll feel each joint, looking for swelling, warmth, and range-of-motion limitations.
Lab tests
Blood work helps confirm the picture. Common markers include:
- ESR & CRP: General inflammation markers.
- Rheumatoid factor (RF): Positive in ~70% of RA cases.
- Anti-CCP antibodies: Highly specific for RA; a positive result can predict aggressive disease.
- ANA: Checked when other autoimmune conditions are suspected.
Imaging
Traditional X-rays reveal joint space narrowing and erosions, while ultrasound or MRI can spot early synovitis that's invisible on plain film.
When to see a rheumatologist?
If joint pain and swelling linger beyond six weeks, or if you notice systemic symptoms like unexplained fatigue, book an appointment. Early specialist care can halt damage before it starts.
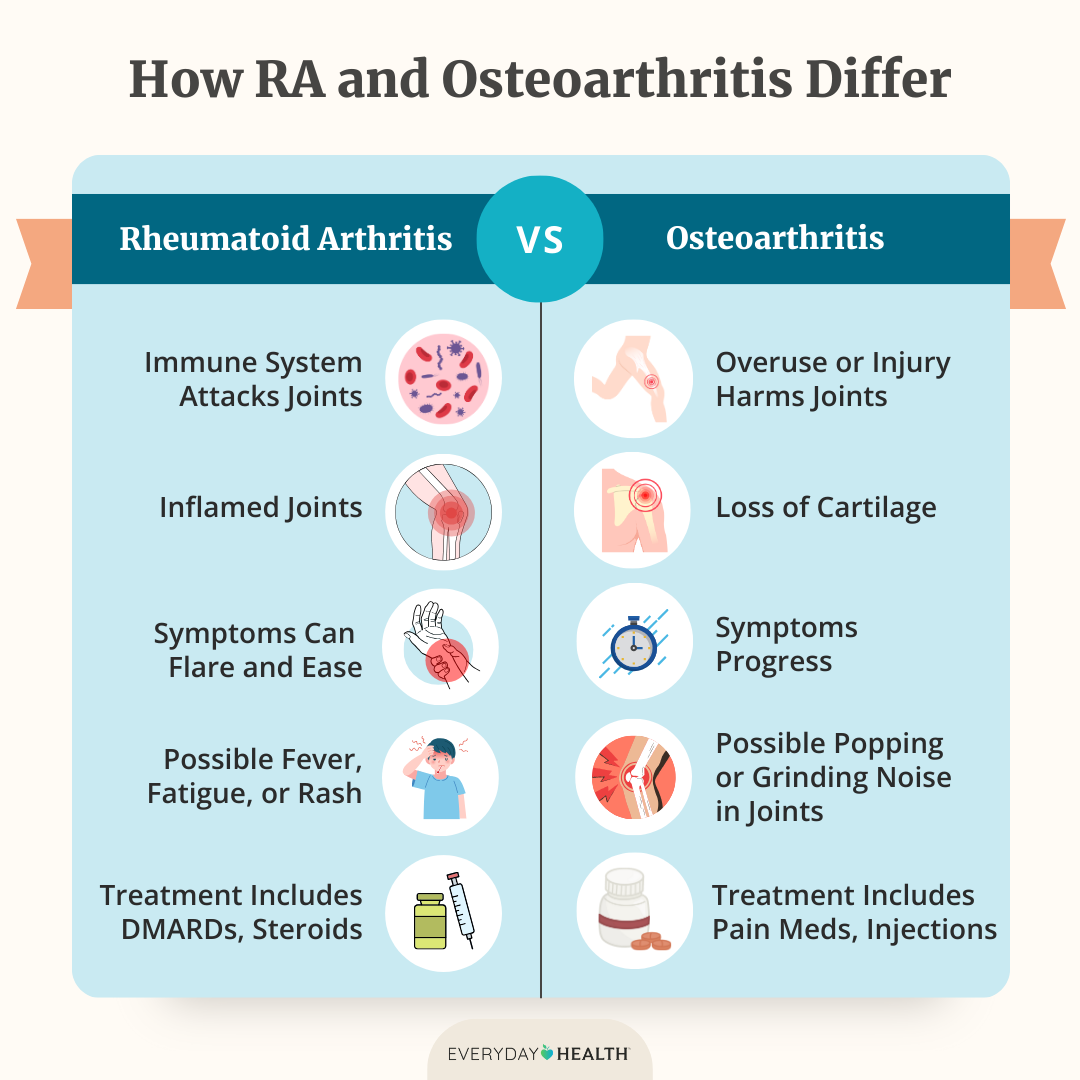
Inflammatory vs Osteoarthritis
Here's a side-by-side snapshot that makes the differences crystal clear:
| Feature | Inflammatory Arthritis (incl. RA) | Osteoarthritis |
|---|---|---|
| Cause | Autoimmune / autoinflammatory attack on synovium | Mechanical wear-and-tear of cartilage |
| Onset | Sudden, weeks to months | Gradual, years |
| Morning stiffness | >30min, improves with movement | <30min, worsens with activity |
| Systemic signs | Fever, fatigue, rash possible | Usually absent |
| Imaging | Erosions, effusion, synovial thickening | Joint-space narrowing, osteophytes |
| Treatment focus | Immune suppression (DMARDs, biologics) | Pain control, joint preservation |
Why the distinction matters for treatment
If you're mistakenly told you have just arthritis and handed only ibuprofen, you're missing the chance to start disease-modifying therapy that could keep RA from destroying your joints. The right label guides the right drug.
Patient story
Emily, 48, thought her hand pain was classic age-related osteoarthritis. After six months of worsening swelling, a friend urged her to see a rheumatologist. Blood tests revealed a high anti-CCP, and she was diagnosed with early RA. Starting methotrexate within weeks prevented the erosions she feared. I wish I'd known the difference sooner, she says.
Best Treatments Available
First-line: NSAIDs & short-term steroids
Nonsteroidal anti-inflammatory drugs (like ibuprofen or naproxen) can tame pain, while a brief course of low-dose prednisone can quiet fierce flare-ups. They're useful bridges, but they don't stop disease progression.
Disease-Modifying Anti-Rheumatic Drugs (DMARDs)
Conventional DMARDs
Methotrexate is the workhorsetaken once a week, it can dramatically reduce joint damage. Sulfasalazine and hydroxychloroquine are often added for a triple therapy approach.
Biologic DMARDs
Targeted biologics like TNF inhibitors (adalimumab, etanercept) or IL-6 blockers (tocilizumab) intervene directly at the inflammatory pathways. They're especially useful when methotrexate alone isn't enough.
Targeted synthetic DMARDs
JAK inhibitors (tofacitinib, upadacitinib) are oral pills that block intracellular signaling, offering an alternative for patients who can't tolerate injections.
Lifestyle adjuncts
Exercise isn't a luxuryit's a prescription. Low-impact activities such as swimming, yoga, or brisk walking keep joints mobile and protect bone density. For personalized [osteoporosis physical therapy](https://medicalhealthzone.com/blog/osteoporosis-physical-therapy "rel=follow referrer" target="_blank") and exercises, consulting specialized therapy plans can greatly help maintain bone health. Omega-3-rich foods (salmon, flaxseed) may also temper inflammation. And, if you smoke, quitting is arguably the single most impactful thing you can do for RA.
Managing side-effects & monitoring
All DMARDs require regular lab checksliver enzymes, kidney function, blood countsto catch problems early. Discuss any new infections or unusual fatigue with your doctor right away.
Personalized care: When aggressive therapy is needed
Not every inflammatory arthritis screams hit hard now. Mild psoriatic arthritis may respond to NSAIDs alone, while aggressive early RA often needs a combination of methotrexate plus a biologic right from the start. As Dr. Ana Martnez, a rheumatology associate professor, explains, Treat-to-target isn't a one-size-fits-all; we aim for remission, but the route depends on disease severity and patient preferences.
Rare Types Explained
Behet's disease
This vasculitic condition can cause painful oral ulcers, eye inflammation, and joint pain. Diagnosis hinges on recurrent mouth sores plus eye or skin lesions; treatment often blends colchicine with low-dose steroids.
SAPHO syndrome
SAPHO stands for Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis. The hallmark is a combination of skin lesions and bone inflammation, especially in the chest wall. NSAIDs and TNF inhibitors are the usual go-tos.
Adult-onset Still's disease
A high-spiking fever, salmon-colored rash, and severe joint pain define this rare form. It can be tricky because labs often show vastly elevated ferritin. IL-1 blockers like anakinra have shown great success.
How they differ from RA
While RA is centered on symmetric small-joint disease, these rarer entities bring extra-articular cluesskin, eyes, or systemic feversthat steer the diagnosis away from classic RA. Treatment may overlap (e.g., biologics) but the choice of drug can shift based on the organ systems involved.
Balancing Benefits & Risks
Early diagnosis = better outcomes
Studies published show that patients who start DMARD therapy within three months of symptom onset are 40% more likely to achieve ankylosing spondylitis remission than those who wait longer.
Risks of untreated inflammation
Beyond joint damage, chronic inflammation raises the risk of cardiovascular disease, osteoporosis, and even depression. It's not just about pain; it's about overall health.
Medication safety vs disease control
Every drug carries potential side effectsliver toxicity with methotrexate, infection risk with biologicsbut the danger of uncontrolled disease often outweighs these concerns. Shared decision-making with your rheumatologist helps you weigh pros and cons.
Practical checklist for you
- Do you notice morning stiffness >30 minutes?
- Is swelling symmetric in hands or feet?
- Have you had any blood tests for RF or anti-CCP?
- Are you seeing a specialist within 6 weeks of persistent symptoms?
- Are you on a treatment plan that aims for remission, not just pain relief?
If you tick most of the boxes, you're on the right track. If not, consider booking that appointmentyou deserve clarity.
Credible Resources Guide
When you're navigating a confusing medical maze, reliable sources are your compass. Here are a few you can trust:
- Hospital for Special Surgery (HSS): Offers detailed patient guides on each type of inflammatory arthritis.
- Mayo Clinic: Clear symptom checklists and drug side-effect profiles.
- Arthritis & Rheumatology (2024) journal articles: For the latest data on biologics and JAK inhibitors.
- American College of Rheumatology (ACR) guidelines: Gold-standard recommendations for diagnosis and treatment.
Feel free to explore these sites; they're regularly updated and written by experts with no hidden agendas.
Conclusion
Inflammatory arthritis is a family of immune-driven joint diseases, and rheumatoid arthritis is its most common, but not sole, member. By recognizing the core signs, understanding how diagnosis works, and knowing the spectrum of treatmentsfrom NSAIDs to biologicsyou can take control of your health journey.
If you've experienced joint pain, stiffness, or any of the symptoms discussed, don't wait. Talk to a rheumatologist, get the right tests, and explore the treatment options that fit your life. And hey, if you have stories or questions, drop a comment belowwe're all in this together.
FAQs
What is the main difference between inflammatory arthritis and rheumatoid arthritis?
Inflammatory arthritis is an umbrella term for several immune‑driven joint diseases; rheumatoid arthritis (RA) is the most common specific type within that group.
How can I tell if my joint pain is inflammatory or osteoarthritis?
Inflammatory arthritis typically causes morning stiffness lasting >30 minutes that improves with movement, plus possible systemic symptoms; osteoarthritis pain worsens with activity and improves with rest, with minimal morning stiffness.
Which tests confirm rheumatoid arthritis?
Blood tests for rheumatoid factor (RF) and anti‑CCP antibodies, along with elevated ESR or CRP, help confirm RA; imaging such as X‑ray, ultrasound, or MRI can show early erosions or synovitis.
What are the first‑line treatments for inflammatory arthritis?
NSAIDs and short‑term low‑dose steroids are used for symptom control, while disease‑modifying anti‑rheumatic drugs (DMARDs) like methotrexate are started early to halt joint damage.
When should I see a rheumatologist for suspected rheumatoid arthritis?
If joint swelling or pain persists longer than six weeks, especially with morning stiffness, systemic signs, or a positive blood test, schedule an appointment with a rheumatologist promptly.