If your ankles or calves have started looking a little puffier, you might be wondering, Is this something serious or just a harmless sideeffect of my new shoes? In the next few minutes well walk through the most common reasons behind peripheral edema, show you how clinicians separate one cause from another, and give you a quick checklist you can use at home. By the end, youll know whether a simple lifestyle tweak will do the trick or if its time to call your doctor.
Well also demystify tricky terms like pitting vs. nonpitting edema, explain why a systematic workup matters for safety, and share practical tips for managing swelling while you wait for a professional diagnosis. Lets dive in together.
Why Diagnosis Matters
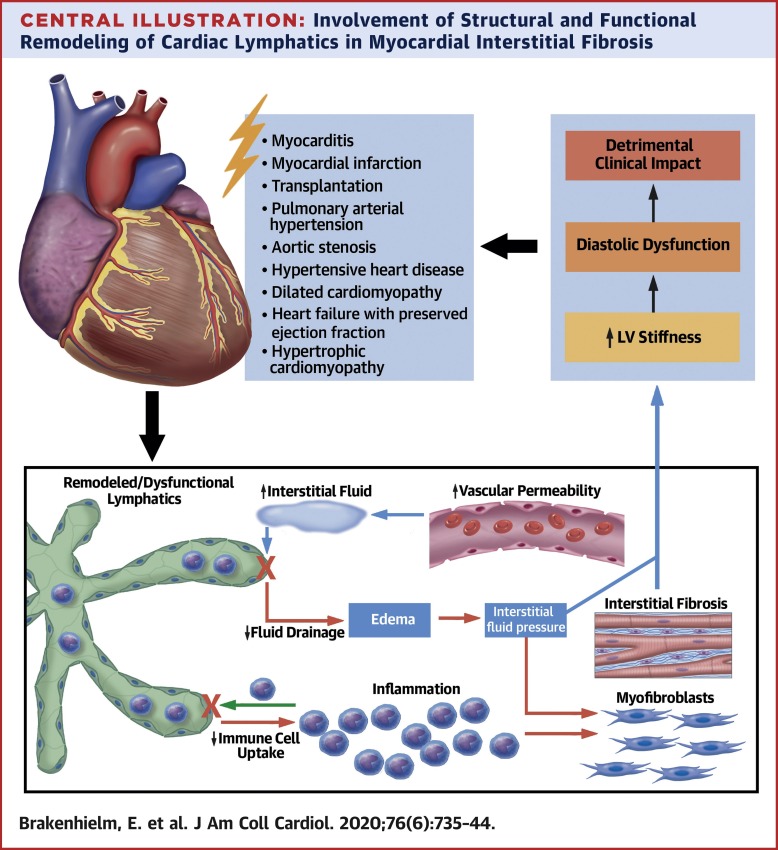
Peripheral edema is a symptom, not a disease. Its the bodys way of flagging that something in the circulatory, renal, hepatic, or lymphatic system isnt quite right. Getting the differential diagnosis right means youll avoid unnecessary medications, prevent complications, and get the right treatment faster.
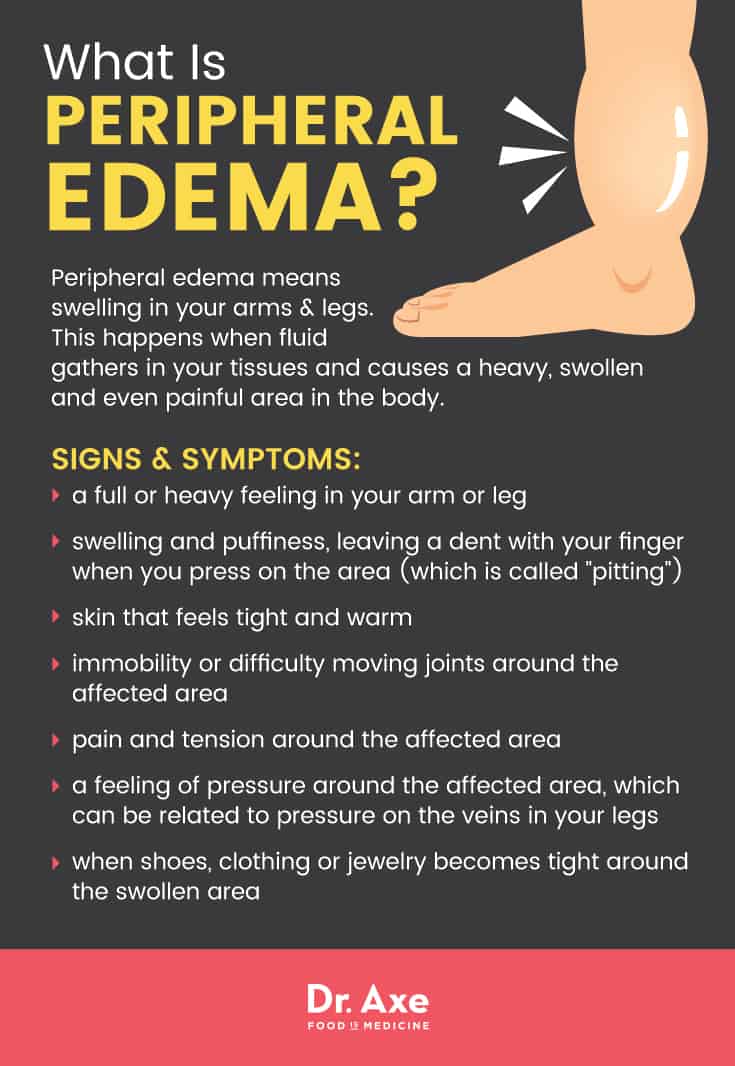
What is peripheral edema?
In plain words, its fluid accumulation in the tissues of the arms, legs, or feet. If you press a fingertip into the swollen area and a dent stays for a few seconds, thats pitting edema. If the skin feels doughy and the dent disappears instantly, youre looking at nonpitting edema.
How the differential guides treatment & safety
Each underlying cause has its own treatment pathway. For example, swelling from heart failure often improves with diuretics and lowsalt diet, while lymphedema may need compression garments and specialized physiotherapy. Knowing the cause helps you choose the safest, most effective peripheral edema treatment.
Core Cause Categories
| Category | Typical Presentation | Key RedFlag Clues | Related Keywords |
|---|---|---|---|
| Cardiovascular (CHF, rightsided heart failure) | Bilateral, pitting, worse at night | Shortness of breath, orthopnea, jugular venous distension | peripheral oedema heart failure |
| Renal / Hepatic (Nephrotic syndrome, cirrhosis) | Generalized, may be nonpitting | Foamy urine, ascites, jaundice | peripheral edema causes |
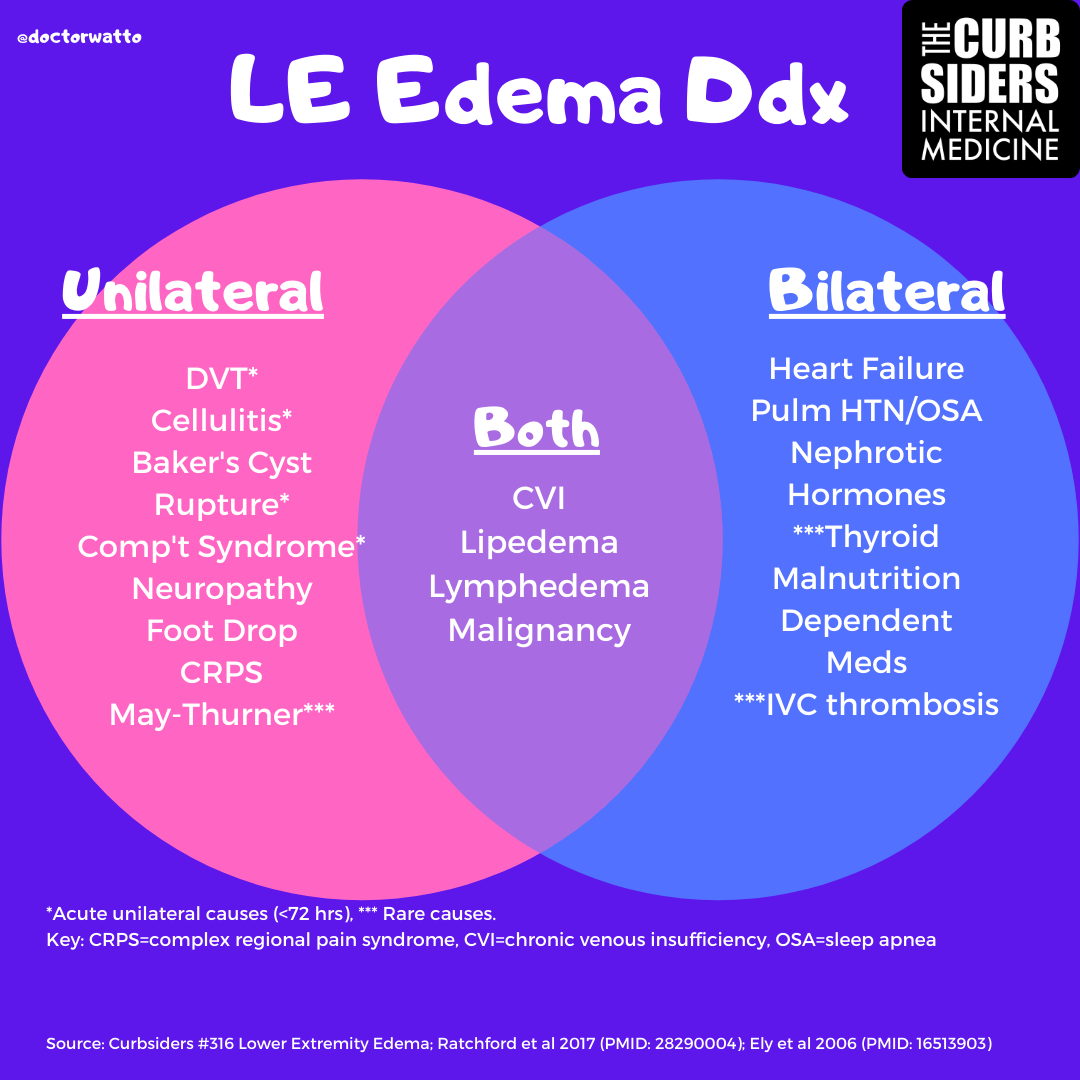
| Venous / Lymphatic (CVI, DVT, lymphedema) | Unilateral or asymmetric, may be nonpitting | Skin discoloration, calf tenderness, warmth | lower limb swelling differential diagnosis |
| Medicationinduced (CCBs, NSAIDs, steroids) | Sudden symmetric swelling | Recent drug change, dose increase | peripheral edema treatment |
| Endocrine / Metabolic (Hypothyroidism, malnutrition) | Soft, nonpitting, cold skin | Weight gain, sluggishness, dry hair | pitting edema causes |
| Local / Traumatic (Cellulitis, hematoma) | Focal, painful, possibly warm | Fever, recent injury | unilateral pitting edema differential diagnosis |
These categories cover the majority of cases youll encounter in primary care or urgentcare settings. Each has a distinct redflag that nudges clinicians toward the right diagnostic pathway.
Clinical Assessment Steps
History taking checklist
- When did the swelling start? Sudden vs. gradual.
- Is it worse at the end of the day or after standing?
- Any recent medication changes? (think calciumchannel blockers, NSAIDs)
- Do you have shortness of breath, chest pain, or cough?
- Any history of heart, kidney, liver disease, or recent travel?
Physical exam pearls
Pitting test
Press a firm fingertip into the swollen area for about 5 seconds. If a dent (grade14) remains, youre dealing with pitting edema. A quick visual can be added to a chart for patients to selfassess.
Systemic clues
- Jugular venous distension points toward cardiac overload.
- Crackles in the lungs another heart failure hint.
- Abdominal fluid (ascites) suggests liver or severe kidney disease.
- Skin changes (hyperpigmentation, ulceration) think chronic venous insufficiency.
Basic bedside tools
Most doctors start with a few labs:
- BNP or NTproBNP for heart failure.
- Serum albumin, creatinine, and urine protein for renal causes.
- Thyroidstimulating hormone (TSH) if hypothyroidism is suspected.
- Duplex ultrasound when DVT or venous reflux is on the radar.
When to order advanced imaging
If you notice rapid unilateral swelling, extreme pain, or signs of infection, the doctor may request a CT or MRI to rule out deepvein thrombosis or a hidden mass. Those are redflag scenarios you dont want to ignore.
Deep Dive Diagnoses
Congestive Heart Failure (CHF)
CHF raises hydrostatic pressure in the veins, pushing fluid out into the tissuesclassic pitting edema. Labs usually show BNP>100pg/mL, and an echocardiogram will confirm reduced ejection fraction. Treatment usually involves diuretics, ACE inhibitors, or ARBs. For patients and clinicians interested in related recovery and treatment options after valve procedures, consider reading about heart valve recovery, which covers postoperative care and monitoring that can influence fluid status.
Chronic Venous Insufficiency (CVI) & DVT
CVI leads to blood pooling in the lower limbs, creating swelling that can be pitting or nonpitting. A unilateral presentation, especially with calf tenderness, should raise suspicion for DVT. Duplex ultrasound is the gold standard showed it catches >95% of cases.
Compression stockings (3040mmHg) help reduce the fluid buildup, but theyre not a substitute for treating an underlying clot.
MedicationInduced Edema
Several common meds act like a sponge:
- Calciumchannel blockers (amlodipine, nifedipine) they dilate arterioles, raising capillary pressure.
- NSAIDs they reduce kidney perfusion, leading to fluid retention.
- Systemic steroids cause sodium and water retention.
When a drug is the culprit, a careful taper or switch (under physician guidance) usually resolves the swelling within days to weeks.
NonPitting Edema (Lymphedema, Myxedema)
Lymphedema feels soft and doughy. It often follows cancer surgery, radiation, or chronic infection. Lymphoscintigraphy can map the blockage, but initial management focuses on compression therapy, manual lymphatic drainage, and skin care.
Myxedema, caused by severe hypothyroidism, presents with a waxy, nonpitting swelling on the face, hands, and feet. A simple TSH test will confirm the diagnosis, and thyroid hormone replacement reverses the edema.
Renal & Hepatic Causes
Nephrotic syndrome floods the bloodstream with proteinpoor fluid, leading to generalized edema that can be both pitting and nonpitting. Urine protein >3.5g/day and low serum albumin are the hallmarks.
Cirrhosis creates portal hypertension, dropping oncotic pressure and causing ascites plus lowerleg swelling. Treating the liver disease and using diuretics (spironolactone + furosemide) helps, but the underlying hepatic issue must be addressed.
Decision Tree Guide
Quick Flowchart
- Bilateral? Yes go to step2. No consider unilateral causes (DVT, cellulitis, lymphedema).
- Pitting? Yes think cardiac, renal, medicationinduced. No consider lymphatic, hypothyroid, hepatic.
- Systemic symptoms? Shortness of breath, cough heart or lung. Abdominal swelling liver/kidney.
- Recent drug changes? Yes medicationinduced.
- Lab results? Elevated BNP heart failure; low albumin nephrotic; high TSH hypothyroidism.
- Imaging? Duplex ultrasound positive DVT/CVI; echocardiogram abnormal CHF.
Feel free to print this checklist and keep it on your fridge. Its a handy selfscreen tool, but remember: its not a substitute for a professional evaluation.
Management Strategies
General measures
- Elevate legs above heart level for 1520minutes, 34 times daily.
- Follow a lowsodium diet (2g per day).
- Stay activeshort walks improve venous return.
- Wear loosefitting clothing to avoid constriction.
Conditionspecific treatments
Heart failure
Loop diuretics (furosemide), ACE inhibitors, and lifestyle changes are firstline. Monitoring weight daily helps catch fluid shifts early.
Venous insufficiency
Graduated compression stockings, calfmuscle exercises, and, when needed, venous ablation procedures.
Medicationinduced
Discuss alternatives with your prescriber. Often a switch to a different antihypertensive (e.g., an ARB without calciumchannel blocker) clears the edema.
Lymphedema
Complete decongestive therapy (manual drainage, compression bandaging, exercise) under a certified therapist.
Hypothyroidism
Levothyroxine replacement normalizes TSH and gradually reduces the myxedema.
Followup & redflag monitoring
Call your doctor right away if you notice:
- Rapid swelling of one leg.
- Pain, redness, or warmth.
- Shortness of breath that worsens at night.
- Sudden weight gain of >2kg in a day.
These signs may indicate infection, a clot, or worsening heart failure.
Conclusion
Peripheral edema is a symptom with many possible rootsfrom a tired heart to a new medication, from liver disease to a blocked lymphatic channel. By taking a systematic history, performing a focused physical exam, and ordering targeted labs, you can quickly narrow the peripheral edema differential diagnosis and land on the right treatment plan.
Use the decisiontree checklist we shared, keep an eye on any redflag changes, and dont hesitate to reach out to your healthcare provider if swelling feels new, painful, or is getting worse. Your body is sending you a message; listening to it can make all the difference.
Have you ever dealt with mysterious leg swelling? Share your story in the comments, or ask any questions you still havewere here to help you navigate it together.
FAQs
What are the main causes of peripheral edema?
Peripheral edema is caused by conditions affecting cardiovascular, renal, hepatic, lymphatic systems, medications, endocrine disorders, or local trauma. Common causes include congestive heart failure, chronic venous insufficiency, nephrotic syndrome, lymphedema, hypothyroidism, and medication side effects.
How can pitting and non-pitting edema help differentiate the cause?
Pitting edema leaves a dent when pressed and is typically seen in heart failure, renal disease, and medication-induced swelling. Non-pitting edema feels doughy and is common in lymphedema and severe hypothyroidism (myxedema).
When should I seek urgent medical care for peripheral edema?
Urgent care is needed if swelling is sudden or severe, especially if unilateral with pain, redness, or warmth, which could indicate deep vein thrombosis or infection, or if accompanied by shortness of breath or rapid weight gain.
What diagnostic tests are important in evaluating peripheral edema?
Key tests include BNP/NT-proBNP for heart failure, serum albumin and urine protein for renal causes, TSH for thyroid function, and duplex ultrasound for DVT or venous insufficiency.
What general measures can help manage peripheral edema at home?
Elevating legs above heart level multiple times daily, following a low-sodium diet, staying active with short walks, and avoiding constrictive clothing can reduce swelling while awaiting diagnosis.