What Is Decorticate?
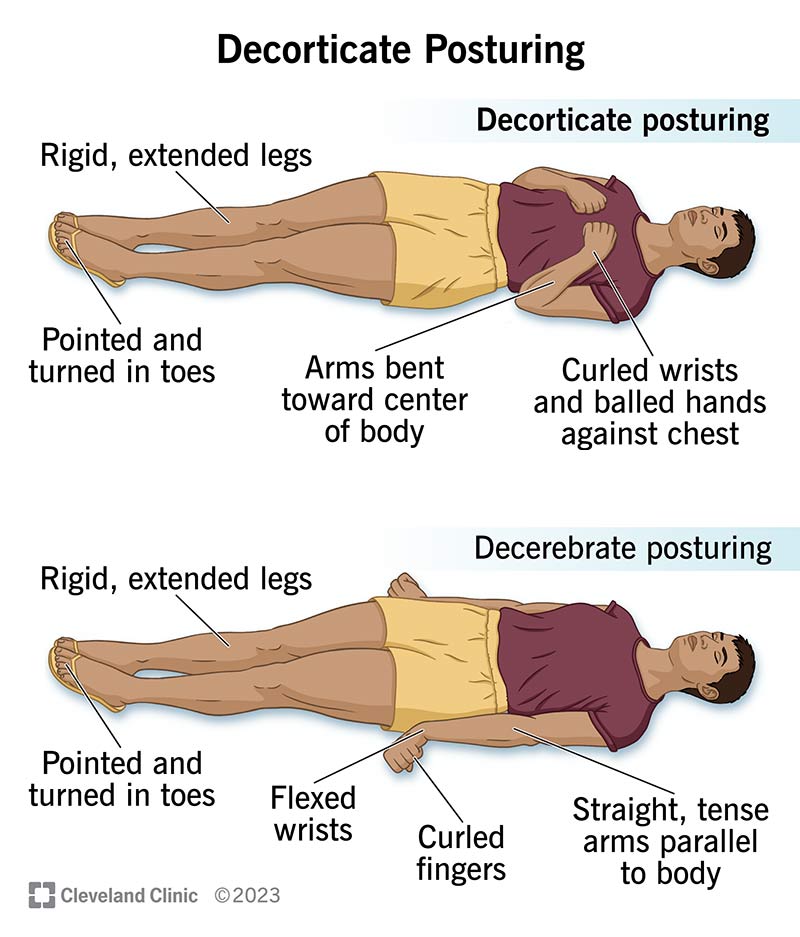
Decorticate posturing is the classic fisted hands, flexed elbows, and straight legs picture you might see in a textbook. The arms are tightly bent at the elbows, the wrists are flexed, and the legs are extended with the feet turned inward. This pattern means the injury is somewhere above the red nucleustypically in the cerebral cortex, thalamus, or internal capsule.
Why does it happen? The corticospinal tract gets interrupted before it reaches the red nucleus, so the brain cant send the usual inhibitory signals to the spinal cord. The result? A reflexive, protective flexion of the upper limbs.
What Is Decerebrate?
Decerebrate posturing looks dramatically different: both the arms and legs are fully extended, the wrists are flexed, and the neck is arched backward. This posture signals damage below the red nucleus, often involving the midbrain or pons. In other words, the brainstems reticular formation cant regulate muscle tone, leading to uncontrolled extension.
Because the brainstem controls essential functionsbreathing, heart rate, consciousnessdecerebrate rigidity is a red flag for lifethreatening injury.
Why Is Decerebrate Worse?
Its not just the posture that looks scarier; it reflects deeper damage. Studies from the show that patients with decerebrate posturing have a significantly higher mortality rate (up to 70% in some series) compared to those with decorticate posturing (around 30%). The brainstem houses the cranial nerves that keep us breathing and awake, so when its compromised, the bodys basic lifesupport systems are at risk.
Thats why clinicians treat decerebrate posturing as a medical emergency, often moving straight to aggressive intracranial pressure (ICP) management and, if needed, emergent decompressive craniectomy.
Causes of Decorticate
- Traumatic brain injury (TBI): Severe contusions or hemorrhages in the cerebral hemispheres.
- Stroke: Large ischemic events affecting the cortical or subcortical regions.
- Brain tumors: Mass effect that compresses the corticospinal pathways.
- Infection: Encephalitis or abscesses causing localized swelling.
All these scenarios interrupt the pathway before the red nucleus, leading to the characteristic flexed arms.
Causes of Decerebrate
- Brainstem trauma: Direct impact or concussion that damages the midbrain or pons.
- Massive intracranial pressure: Brain herniation (especially upward transtentorial) that forces the brainstem downward.
- Diffuse axonal injury: Widespread tearing of nerve fibers that compromises deep structures.
- Severe hypoxia: Neardrowning or cardiac arrest can starve the brainstem of oxygen.
Because these injuries affect the core command center of the nervous system, they often lead to rapid deterioration if not addressed immediately.
Prognosis Comparison
| Feature | Decorticate Posturing | Decerebrate Posturing |
|---|---|---|
| Typical Brain Area Affected | Cortex, thalamus, internal capsule | Midbrain, pons (brainstem) |
| 30day Survival Rate | 70% | 30% |
| LongTerm Functional Outcome | Higher chance of meaningful recovery | Often severe disability or vegetative state |
| Typical Interventions | ICP control, medical management | Urgent surgical decompression, aggressive ICP reduction |
The numbers speak for themselves: decerebrate posturing correlates with a poorer prognosis, yet its not an absolute sentence. Prompt, targeted care can still make a difference.
Recognizing the Posture
When youre in the field or bedside, a quick visual checklist helps:
- Arms: Flexed with fists (decorticate) vs. extended and pronated (decerebrate).
- Legs: Extended in both, but note foot positioningturned inward (decorticate) or straight (decerebrate).
- Neck: Neutral in decorticate; hyperextended in decerebrate.
- Pupils: Look for asymmetryoften more pronounced in decerebrate cases.
If the posture is ambiguous, a CT or MRI can pinpoint the lesion level. The imaging will usually reveal a cortical bleed for decorticate or a brainstem shift for decerebrate.
Mnemonic for Quick Recall
Heres a handy mnemonic that many nursing students love: DECCORT / DECBER.
- DECCORT: C = Cortex Decorticate (cortical injury).
- DECBER: B = Brainstem Decerebrate (brainstem injury).
Whenever you see a patients posture, think C or B? Itll help you remember the underlying anatomy.
Managing Each Posture
Decorticate Management
Even though its less dire than decerebrate, decorticate still demands swift action. Heres the typical approach:
- Airway and Breathing: Ensure the patient is protectedintubate if GCS 8.
- ICP Control: Mannitol or hypertonic saline to keep pressure below 20mmHg.
- Blood Pressure Management: Maintain cerebral perfusion pressure (CPP) >60mmHg.
- Surgical Evaluation: Craniotomy for hematoma evacuation if indicated.
Decerebrate Management
When the brainstem is on the line, the stakes are higher:
- Immediate ICP Reduction: Rapid bolus of hypertonic saline, consider barbiturate coma.
- Emergent Decompressive Craniectomy: Often the only way to relieve pressure on the brainstem.
- Ventilation Support: Optimize oxygenation and CO (aim for PaCO35mmHg).
- Neuromonitoring: Continuous EEG and brain tissue oxygen monitoring if available.
Both pathways require tight coordination with neurosurgeons, intensivists, and nursing staff. For patients who also have complex neurological conditions such as atypical Rett syndrome, early specialist involvement can help tailor longterm care plans and rehabilitation goals; learn more about atypical Rett syndrome atypical Rett syndrome.
Rehabilitation & LongTerm Care
Surviving the acute phase is just the first hurdle. Rehabilitation differs based on the original posture:
- Decorticate Survivors: Focus on preventing contractures in flexed limbs, early mobilization, and neuroplasticityfocused therapies.
- Decerebrate Survivors: Emphasis on managing spasticity, ventilator weaning, and intensive physical therapy to regain basic functions.
Family counseling is essential. Understanding that worse doesnt always mean hopeless helps set realistic expectations while preserving hope.
Expert Opinions & Sources
Dr. Lisa Nguyen, a boardcertified neurointensivist at , notes, When I see decerebrate rigidity, my first thought is brainstem at risk. That urgency drives us to act faster, often with surgical decompression, whereas decorticate signals a serious but sometimes more controllable injury.
Guidelines from the American Association of Neurological Surgeons (AANS) and the American Stroke Association (ASA) reinforce these strategies, advocating for rapid ICP monitoring and early neurosurgical consultation when decerebrate posturing is present.
Final Takeaway Summary
So, to bring it all together: decerebrate posturing is generally the worse sign because it indicates brainstem involvement, higher mortality, and a need for aggressive, often surgical, intervention. Decorticate posturing, while still a warning of serious brain injury, usually points to cortical damage that has a relatively better prognosis with prompt medical care.
Whether youre a medical professional, a caregiver, or just someone curious about braininjury signs, remembering the distinctionand the mnemonic C or B?can make a real difference in understanding the urgency of a situation.
Whats your experience with these postures? Have you seen a case where quick recognition changed the outcome? Share your thoughts in the comments, and if you have any questions, dont hesitate to askwere in this together.
FAQs
What is the main difference between decerebrate and decorticate posturing?
Decorticate posturing involves flexed arms and extended legs, indicating damage above the red nucleus (cortex or thalamus). Decerebrate posturing shows fully extended arms and legs, pointing to injury below the red nucleus in the brain‑stem.
Why is decerebrate posturing considered more dangerous?
Because it reflects brain‑stem involvement, which controls vital functions like breathing and consciousness. Damage here leads to higher mortality and often requires urgent surgical intervention.
What are common causes of decorticate posturing?
Typical causes include severe traumatic brain injury, large cortical strokes, space‑occupying brain tumors, and infections such as encephalitis that compress corticospinal pathways above the red nucleus.
How should clinicians initially manage a patient with decerebrate rigidity?
Immediate steps focus on rapid intracranial pressure reduction (hypertonic saline or mannitol), possible emergent decompressive craniectomy, airway protection, and strict ventilation control to maintain adequate oxygenation.
Can a patient with decerebrate posturing recover?
Recovery is possible but less likely; prognosis hinges on how quickly the underlying cause is treated. Early aggressive ICP management and neurosurgical decompression improve the odds of survival and functional outcome.