If youve just learned that the sputum culture from your lungs (or a loved ones) shows Burkholderia cepacia, youre probably feeling a mix of confusion, worry, and a flood of questions. The short answer is:there is a treatment plan that can help keep the infection under control, protect lung function, and give you peace of mind. Below youll find everything you need to knowfrom the science behind the bug to practical daily tipsdelivered in a friendly, letstalkovercoffee style.
Why it matters
What is the Burkholderia cepacia complex?
The Burkholderia cepacia complex (often shortened to Bcc) is a group of related bacteria that love to thrive in the moist, mucusfilled airways of people with cystic fibrosis (CF). While most of us have never heard the name, in the CF community its a wellknown foe because it can cause rapid lung damage and, in severe cases, a lifethreatening condition called Cepacia syndrome.
How does Bcc affect the lungs?
Think of the cystic fibrosis airways as a garden thats constantly being watered. The extra water (thick mucus) creates the perfect environment for Bcc to grow. Once it settles in, it releases enzymes that inflame the airway walls, destroy tiny airway structures, and make it harder for the lungs to move air in and out. The result? A faster decline in FEV (the measure of how much air you can forcefully exhale) and more frequent exacerbations that land you in the hospital.
Key statistics to keep in mind
- About 510% of people with CF are chronically colonized with Bcc.
- Chronic infection can shorten median survival by roughly 510years compared with noninfected peers.
- Patients who develop Cepacia syndrome have a mortality risk of up to 30% within the first month of onset.
Treatment guidelines
Firstline antibiotic strategies
Guidelines from the Cystic Fibrosis Foundation (CFF) recommend an aggressive, multidrug approach because Bcc is naturally resistant to many antibiotics. A typical regimen starts with:
- IV ceftazidime (a lactam) plus meropenem or imipenem to hit the bacteria hard.
- Simultaneous oral trimethoprimsulfamethoxazole (TMPSMX) for broader coverage.
- Followup inhaled antibiotics (e.g., inhaled tobramycin or inhaled aztreonam) for longterm suppression.
These drugs are chosen based on the specific antibiogram your CF center sends after the cultureso the exact combo can vary.
Tailoring therapy to sensitivity patterns
Every Bcc infection is a little different. Labs test each isolate against a panel of antibiotics and report the Minimum Inhibitory Concentrations (MICs). Your care team will look for the lowest MICs, then build a regimen that maximizes synergy (the idea that two drugs together work better than each alone). According to a 2024 review in , personalized combos improve eradication rates by up to 30%.
How long should treatment last?
There are basically two phases:
- Intensive phase: 23weeks of IV antibiotics, usually given in the hospital or via home infusion.
- Maintenance phase: 36months of inhaled suppressive therapy, sometimes combined with lowdose oral agents.
If sputum cultures stay negative after the intensive phase, some clinicians may shorten the maintenance periodbut most prefer a minimum of three months to keep the bacteria from rebounding.
Standard vs. individualized regimens
| Regimen | Route | Typical Length | Pros | Cons |
|---|---|---|---|---|
| IV lactam + meropenem | IV | 1421days | Rapid bacterial kill | Hospital stay/IV line risks |
| Oral TMPSMX + inhaled tobramycin | Oral + inhaled | 3090days | Outpatient friendly | Potential resistance, sideeffects |
Benefits and risks
Potential benefits of aggressive therapy
When the regimen works, youll notice:
- Reduced cough and sputum volume.
- Stabilizationor even a modest improvementin FEV.
- Fewer hospital admissions, meaning more time for school, work, or hobbies.
Common sideeffects and longterm risks
Every powerful antibiotic cocktail carries a price:
- Nephrotoxicity: Some lactams can stress the kidneys; regular blood work is a must.
- Ototoxicity: Aminoglycosides (like tobramycin) can affect hearing, especially with prolonged use.
- Clostridioides difficile infection: Broadspectrum agents disrupt gut flora, raising the risk of a nasty diarrhea.
- Drug interactions: Many newer CFTR modulators (e.g., ivacaftor) are metabolized by the same liver enzymes as some antibiotics, so dosing may need adjustment.
How to monitor safely
Ask your team to set up a simple checklist:
- Baseline serum creatinine and weekly followup.
- Monthly audiogram if youre on aminoglycosides.
- Weekly sputum cultures to watch for recolonization.
- Blood counts to catch bonemarrow suppression early.
Special scenarios
Lung transplant considerations
For some, a transplant becomes the best longterm solution. However, chronic Bcc infection can complicate eligibility. Studies show that patients who are cleared (negative cultures for at least six months) before transplant have significantly better postoperative outcomes. If a transplant is on your radar, discuss an aggressive eradication plan with your transplant pulmonologist early.
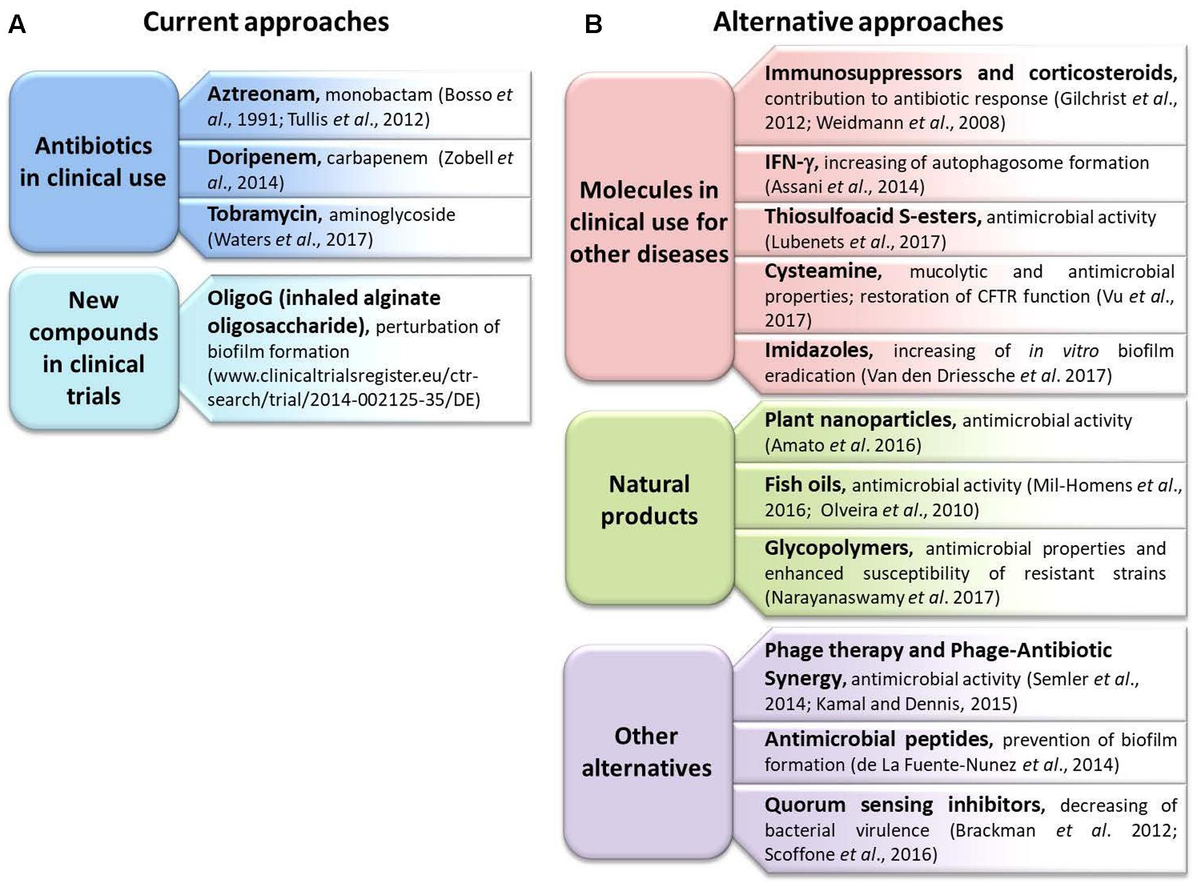
Phage therapy the frontier
Phage therapy uses viruses that specifically attack bacteria. A 2024 article in described a small trial where customtailored phage cocktails reduced Bcc load in 3 out of 5 participants. Its still experimental, but for those who have exhausted antibiotics, its an option worth asking about.
Managing Cepacia syndrome
If you suddenly develop high fever, rapid lung function loss, and bloodtinged sputum, you could be facing Cepacia syndromean emergency. The recommended response is highdose IV lactam plus an aminoglycoside, plus supportive ICU care. Time is critical, so have an emergency action plan ready (e.g., a onepage what to do card in your medical bag).
Everyday precautions
Infectioncontrol at home and clinic
Even after successful treatment, Bcc can linger on surfaces. Simple habits can dramatically lower reinfection risk:
- Separate nebulizer kits for Bccpositive days.
- Use a dedicated handwashing sink or hand sanitizer before/after airway clearance.
- Wear a surgical mask in crowded clinics, especially during exacerbations.
- Ask your CF center about isolation rooms for highrisk visits.
For surface disinfection and preventing spread of other pathogens that can worsen lung disease, consider guidance on how household disinfectants act against common viruses and bacteria for example, whether certain products can inactivate norovirus-like agents on surfaces.
Travel, school, and work tips
Planning a trip? Pack extra supplies, keep your antibiotics on hand, and let the airline know you have a medical condition (they can provide a preboard option). In school or work, a brief note from your doctor explaining the need for maskuse and occasional stayhomewhensick days can keep peers informed without oversharing.
Quickreference Do / Dont list
Do: Clean nebulizer parts daily, keep a copy of your latest sputum culture, schedule routine labs.
Dont: Share airway devices, skip a dose of oral antibiotics, ignore new or worsening symptoms.
Spotting symptoms
Early warning signs
Most patients notice a subtle change first:
- Increase in cough frequency.
- Thicker, greenyellow sputum.
- Lowgrade fever (under 101F).
- Feeling more breathless than usual during routine activities.
Redflag alarms that need urgent care
If any of these appear, call your CF team or head to the nearest emergency department:
- Sudden drop in FEV >10%.
- Highgrade fever (>101F) lasting more than 24hours.
- Hemoptysis (coughing up blood).
- Severe chest pain or rapid heart rate.
Life expectancy
What the numbers say
Data from the CFF Registry (2023) indicate that median survival for people with chronic Bcc infection is roughly 1015years after the first positive culture, compared with 2025years for those never infected. However, these are averagesindividual outcomes can vary wildly based on early detection, treatment adherence, and overall health.
How treatment choices influence longevity
Patients who achieve early eradication (negative cultures within three months) often enjoy a survival curve similar to noninfected peers. Conversely, persistent infection without aggressive management is linked to faster lung decline and earlier transplant need. The takeaway? Prompt, personalized therapy really does matter.
Realworld story
Emilys twoyear remission journey
Emily, a 22yearold university student, was diagnosed with Bcc after a routine sputum test. Her initial reaction was What now? She immediately met with her CF multidisciplinary team, who crafted a 21day IV combo of ceftazidime and meropenem plus oral TMPSMX. While in the hospital, Emily kept a journal of how the treatment felt the IV line was a bit of a nuisance, but hearing my lungs clear was worth it. After discharge, she switched to inhaled tobramycin twice daily for six months.
Six months later, her cultures were still negative. Emily now follows a quarterly sputum check, does her airway clearance twice a day, and keeps a spare nebulizer kit by the bedside. Two years after that scary culture, she reports a stable FEV and a thriving social life. Her story illustrates that with a proactive team and diligent selfcare, Bcc doesnt have to be a life sentence.
Key takeaways from Emilys experience
- Dont wait for symptoms to worsenact on the first positive culture.
- Embrace the allhandsondeck approach: IV, oral, and inhaled antibiotics together.
- Stay organized; a simple journal can track sideeffects and motivate adherence.
Conclusion
Living with Burkholderia cepacia cystic fibrosis treatment can feel like navigating a maze, but the map is clearer than ever. A personalized, guidelinebacked antibiotic planpaired with vigilant monitoring, thoughtful daily precautions, and a supportive care teamoffers the best chance to keep the infection at bay, preserve lung function, and maintain quality of life.
Remember, you dont have to face this alone. Talk openly with your CF specialists about the latest guidelines, ask about emerging options like phage therapy, and share your concerns with friends and family who can help you stay on track. If you or someone you love just received a Bcc diagnosis, reach out today and start the conversation that could change the trajectory of your health.
FAQs
What is the first-line treatment for Burkholderia cepacia in cystic fibrosis?
First-line treatment typically includes IV ceftazidime plus meropenem or imipenem, often combined with oral trimethoprim-sulfamethoxazole.
How long does antibiotic treatment last for Burkholderia cepacia?
Intensive IV therapy usually lasts 2–3 weeks, followed by 3–6 months of inhaled or oral suppressive therapy.
Can Burkholderia cepacia be cured in cystic fibrosis?
Complete eradication is challenging, but aggressive therapy can achieve remission and improve lung function in some patients.
What are the risks of Burkholderia cepacia treatment?
Risks include nephrotoxicity, ototoxicity, Clostridioides difficile infection, and drug interactions with CFTR modulators.
How is treatment tailored for Burkholderia cepacia?
Treatment is based on antibiotic sensitivity testing, aiming for synergistic combinations to maximize effectiveness.