You need a fast, reliable way to decide whether a patient with infection is heading toward sepsis and you dont have time to leaf through a textbook. Below youll find the exact criteria, calculators and pros/cons of every major sepsis scoring tool, so you can pick the right one in seconds.
Because every tool has strengths and blind spots, well break down diagnostic vs. prognostic scores, show realworld examples, and give you a printable chart you can stick on the wall or embed in your EMR today.
What Are Scoring Tools
Definition
A sepsis scoring tool quantifies infectionrelated organ dysfunction to aid diagnosis and risk stratification. In plain language, it turns a muddle of vitals and labs into a simple number that tells you how worried should I be?
Key Purposes
- Early detection of sepsis before it spirals.
- Guiding antimicrobial therapy and fluid resuscitation.
- Prioritizing ICU versus ward admission.
- Providing data for qualitymetric reporting and research.
Diagnostic vs Prognostic Scores
Diagnostic Scores
These are meant to flag a possible sepsis case. They focus on inflammation, vitalsign changes, and simple labs.
- SIRS criteria temperature, heart rate, respiratory rate, whitebloodcell count.
- NEWS (National Early Warning Score) adds oxygen requirements and level of consciousness.
- PRESEP combines clinical signs with a few lab values for a bedside sepsis suspicion number.
Prognostic Scores
Once sepsis is suspected, prognostic scores estimate the risk of organ failure or death. They are the tools you reach for when you need to decide ICU or not?
- SOFA score evaluates six organ systems (respiratory, coagulation, liver, cardiovascular, CNS, renal).
- qSOFA score the quick threepoint version for nonICU settings.
- SPEED, MEDS, PIRO more specialized models that incorporate comorbidities, infection source, and patient response.
| Score | Type | Key Criteria | Typical Setting | Best For |
|---|---|---|---|---|
| SIRS | Diagnostic | Temp>38C or<36C, HR>90, RR>20, WBC>12k/L or<4k/L | ED/ward | Rapid screen |
| NEWS | Diagnostic | Respiratory rate, SpO, O use, BP, HR, Temp, consciousness | Hospital, prehospital | ICU admission decision |
| PRESEP | Diagnostic | Combination of vitals, lactate, CRP | ED | Early detection |
| SOFA | Prognostic | Resp, coag, liver, CV, CNS, renal (04 each) | ICU | Organfailure tracking |
| qSOFA | Prognostic | SBP100mmHg, RR22, altered mentation | NonICU bedside | Mortality risk |
| SPEED | Prognostic | Age, comorbidities, vitals, lactate | ICU | Rapid risk estimate |
| MEDS | Prognostic | Age, terminal illness, septic shock, platelets | ED | Mortality prediction |
| PIRO | Prognostic | Patient, Infection, Response, Organ dysfunction (many variables) | Research/advanced care | Comprehensive risk |
MiniProfiles of Major Tools
SIRS Score
How to Calculate
- Check temperature: >38C or <36C = 1 point.
- Heart rate >90bpm = 1 point.
- Respiratory rate >20/min = 1 point.
- Whitebloodcell count >12k/L or <4k/L = 1 point.
- Two or more points = sepsis suspicion.
RealWorld Example
Imagine a 62yearold man with communityacquired pneumonia. His vitals are 39C, HR 112, RR 24, WBC 14k/L. He scores 4/4 a clear red flag that prompts immediate broadspectrum antibiotics and fluid bolus.
NEWS (National Early Warning Score)
Why Clinicians Love It
Recent research . It captures oxygen use and mental status, which SIRS completely ignores.
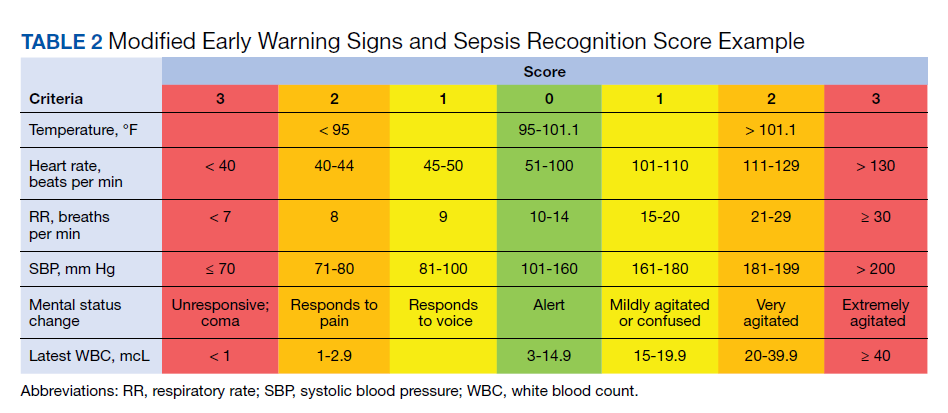
Sample Chart
| Parameter | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|
| Respiratory Rate | 1220 | 911 or 2124 | 8 or 2530 | >30 |
| SpO | 96% | 9495% | 9293% | <92% |
| OSupp. | None | Low flow | High flow | Ventilated |
| SBP | 111219mmHg | 101110 | 91100 | 90 |
| Heart Rate | 5190 | 4150 or 91110 | 111130 | >130 |
| Temperature | 36.138.0C | 35.136.0 or 38.139.0 | 34.035.0 or >39.0 | |
| Consciousness | Alert | New confusion, Voice, Pain | Unresponsive |
qSOFA Score
Exact Criteria
Three bedside items, each worth one point:
- Systolic blood pressure100mmHg
- Respiratory rate22/min
- Altered mentation (GCS<15)
Score2 suggests a high risk of mortality and may trigger a full SOFA assessment.
When qSOFA Misses
Immunocompromised patients often present with normal blood pressure but severe infection. In a study of oncology wards, qSOFA failed to identify 30% of patients who later required ICU care. Thats why many clinicians pair qSOFA with a quick lactate check.
SOFA Score
Breakdown of Six Organs
- Respiratory PaO/FiO ratio
- Coagulation Platelet count
- Liver Bilirubin
- Cardiovascular MAP or vasopressor dose
- CNS Glasgow Coma Scale
- Renal Creatinine or urine output
Each organ scores 04; a rise of 2 points from baseline indicates sepsis3 criteria. For a quick reference on how the SOFA calculation translates individual lab and vitals values into organ scores, keep a laminated chart at the bedside.
RealWorld Application
Take a 48yearold woman with intraabdominal sepsis. Initial SOFA 3 (mild respiratory dysfunction). After 24h shes on norepinephrine, platelets have dropped, and creatinine rose total SOFA 9. The jump of 6 points drives a rapid escalation to the ICU and a review of source control.
Using a Sepsis Score Calculator
Free Online Tools
Websites like host calculators for SIRS, qSOFA, SOFA, and more. You can also download a from the CDC for offline use.
StepbyStep Screenshot Guide
- Open the calculator in your browser or on a mobile device.
- Enter the latest vital signs and lab values.
- Hit calculate. The page instantly displays the total score and risk category.
- Copy the result into the patients chart or EMR note.
Integrating Into an EMR
Most modern EMRs let you embed a web widget or upload a PDF form. To keep it smooth:
- Map each field (e.g., SBP) to an existing data point.
- Set a trigger: if the calculated score2, automatically flag the patient for rapid response.
- Schedule a quarterly audit to ensure the tool is still uptodate with the latest sepsis3 criteria.
Benefits and Risks of Scoring Tools
Benefits
- Standardization Everyone speaks the same language, reducing variability.
- Early detection A high SIRS or NEWS score can prompt antibiotics within the critical golden hour.
- Data collection Scores feed dashboards that help hospitals improve quality metrics.
Risks
- Overtriage A lowspecificity tool may flood the ICU with patients who could stay on the ward.
- Missed atypical presentations Elderly or immunocompromised patients may not meet qSOFA criteria but are still septic.
- Tool fatigue Too many calculators can lead to buttonpushing without genuine clinical judgement.
Case Study: Missed qSOFA
John, a 70yearold with chronic lymphocytic leukemia, presented with a mild fever (38.2C) and normal blood pressure but a lactate of 4mmol/L. qSOFA was 0, yet he rapidly deteriorated. The team learned to pair qSOFA with lactate and a quick SIRS check for highrisk patients.
Choosing the Right Tool for Your Setting
Decision Matrix
| Clinical Setting | Primary Goal | Best Tool(s) |
|---|---|---|
| Emergency Department | Rapid identification | SIRS, NEWS, PRESEP |
| General Ward | Monitor progression | qSOFA + lactate, NEWS |
| Intensive Care Unit | Organfailure tracking | SOFA, SPEED, MEDS |
| Prehospital (EMS) | Brief bedside screen | qSOFA, NEWS (simplified) |
Implementation Roadmap
- Training Conduct a 30minute workshop using real case scenarios.
- Pilot Choose one unit, collect data for two weeks, adjust thresholds if needed.
- Audit Review outcomes (time to antibiotics, ICU transfers) monthly.
- Feedback Loop Encourage staff to report frustrations; iterate the tool or workflow.
Conclusion
Bottom line: Sepsis scoring tools arent onesizefitsall. Use SIRS, NEWS, or PRESEP to spot infection early, then switch to SOFA, qSOFA, SPEED, MEDS or PIRO for risk stratification and ICU decisions. Pick the tool that matches your workflow, back it up with a quick calculator, and regularly audit outcomes thats how a score transforms into saved lives.
What scoring tool do you rely on most in your practice? Share your experiences in the comments, or ask any lingering questions were all in this together.
FAQs
What is the difference between diagnostic and prognostic sepsis scores?
Diagnostic scores (e.g., SIRS, NEWS, PRESEP) identify possible sepsis early, while prognostic scores (e.g., qSOFA, SOFA, MEDS) estimate the risk of organ failure or death once sepsis is suspected.
When should I use qSOFA instead of the full SOFA score?
qSOFA is ideal at the bedside in non‑ICU settings for rapid risk assessment. If a patient scores ≥2, you should follow up with a full SOFA evaluation.
Are there free online calculators for these scoring tools?
Yes—sites like MDCalc provide free calculators for SIRS, qSOFA, SOFA, NEWS, and other tools, and many hospitals offer printable PDFs for offline use.
Can sepsis scoring tools be integrated into the EMR?
Most modern EMRs allow embedding calculators or PDF forms, mapping vital‑sign fields to auto‑calculate scores and trigger alerts when thresholds are met.
What are the main pitfalls of relying solely on a sepsis score?
Scores can over‑triage patients, miss atypical presentations (e.g., immunocompromised patients), and cause “tool fatigue.” Always combine scores with clinical judgment.