What if you could translate a handful of lab numbers into a clear picture of a patients sepsis severity in under two minutes? Thats exactly what the SOFA score sepsis calculator does. Plug in six routine values, click calculate, and you get a score that tells you how likely organ failure is to progressand whether you should call in the ICU team right now.
Lets walk through everything you need to know, from the basic definition to realworld case stories, all in a friendly, coffeechat style. No long histories, no jargon overloadjust straighttothepoint guidance you can use today.
What Is SOFA?
Definition
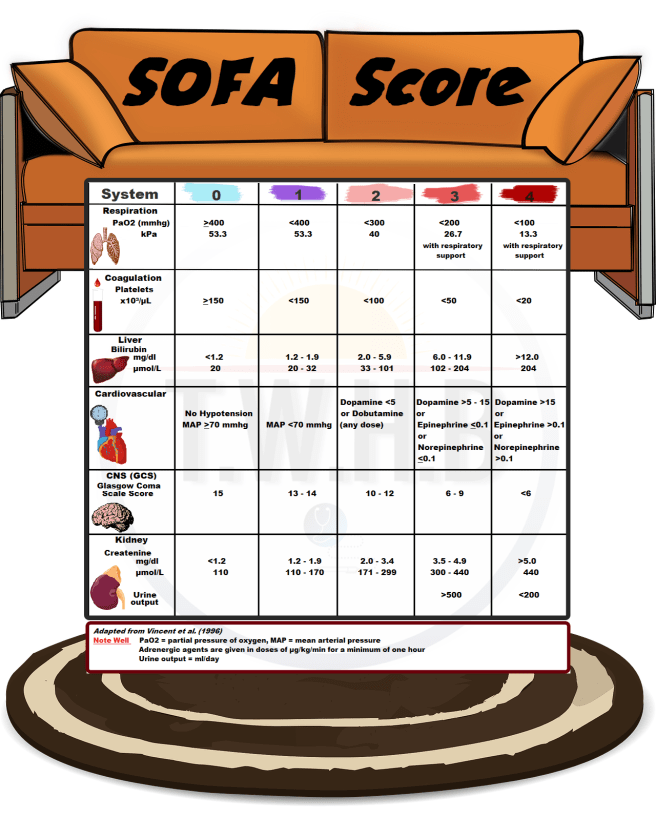
SOFA stands for Sequential Organ Failure Assessment. Its a scoring system that looks at how six organ systems are functioning and assigns each a value from 0 (normal) to 4 (most severe). The total adds up to a number that predicts the risk of mortality from sepsis.
Six Organ Systems
| Organ System | Metric Used | Score Range |
|---|---|---|
| Respiratory | PaO/FiO ratio | 04 |
| Coagulation | Platelet count (10/L) | 04 |
| Liver | Bilirubin (mg/dL) | 04 |
| Cardiovascular | Mean arterial pressure & vasopressor dose | 04 |
| Central Nervous System | Glasgow Coma Scale | 04 |
| Renal | Creatinine (mg/dL) or urine output | 04 |
Why It Matters for Sepsis
The higher the score, the higher the probability that a patient will need intensive care and the greater the mortality risk. Studies on show mortality climbs from roughly 10% at a score of 04 to over 70% when the score reaches 10 or more. In short, the SOFA score is a quick, evidencebased alarm bell.
Using the Calculator
Where to Find It
There are several reliable, free webbased calculators. The most reputable are:
All three are clinically vetted, mobileresponsive, and free to use. Pick the one you like best and bookmark it for quick access during rounds.
Data Youll Need
Before you start, make sure you have the most recent values for:
- Arterial oxygen (PaO) and FiO
- Platelet count
- Total bilirubin
- Mean arterial pressure (MAP) and any vasopressor dose
- Glasgow Coma Scale (GCS) score
- Serum creatinine or urine output (mL/hr)
All of these are typically pulled from the electronic health record within minutes, so you dont need any extra tests.
StepbyStep Walkthrough
Heres how a typical calculation looks on MDCalc (feel free to follow along on your screen):
- Open the calculator and select Enter values manually.
- Input the PaO/FiO ratioif the patient is on room air, FiO is 0.21.
- Enter the platelet count; the tool automatically maps it to a score.
- Type the bilirubin level, MAP, vasopressor dose, GCS, and creatinine or urine output.
- Press Calculate. The total SOFA score appears instantly, along with a brief interpretation.
Quick tip: If MAP is below 70mmHg and youre already on norepinephrine, the calculator will add extra points for the vasopressor doseso doublecheck the infusion rate.
Interpreting the Results
Score Ranges
Think of the total as a traffic light:
- 04: Green low risk, continue routine monitoring.
- 59: Yellow moderate risk, consider ICU consult and closer labs.
- 10: Red high risk, act fast: start broadspectrum antibiotics, secure the airway if needed, and alert the ICU team.
According to the validation data on , a score of 6 predicts about a 30% mortality risk, while a score of 12 jumps to over 80%.
Changing Over Time
SOFA isnt a onetime measurement. The original Sepsis3 definition suggests calculating the baseline at admission, then reassessing at 24hours and again at 48hours. An upward trendsay from 5 to 8signals worsening organ dysfunction and should trigger escalation of care.
When to Take Action
Whenever the score climbs into the yellow or red zones, follow a simple checklist:
- Notify the ICU attending.
- Start or broaden antimicrobial coverage per guidelines.
- Consider vasopressor support if MAP remains <65mmHg.
- Reorder labs (lactate, cultures, repeat ABG) to track response.
- Document the score trend in the chart for the whole team.
Benefits and Risks
Benefits
Using the SOFA score sepsis calculator gives you an objective number that everyone can understand, streamlines communication, and aligns you with international research standards. Its also a handy tool for teaching residentsshow them how each organ system contributes to the overall picture.
Potential Pitfalls
Numbers cant replace bedside judgment. Relying solely on a calculator may cause you to miss nuances such as a patients frailty, comorbidities, or rapid clinical changes that havent yet shown up in labs. Also, different labs may have slightly varying reference ranges, which can affect the scoring.
Mitigating the Risks
Think of the SOFA score as a second opinion from your data. Always pair it with a thorough physical exam and the patients overall trajectory. If a lab value is missing, use the worstcase default (the highest possible score for that organ) and clearly note the limitation in the chart.
SOFA vs. qSOFA vs. APACHE
Key Differences
| Score | Setting | Parameters | Time to Compute | Predictive Accuracy (AUC) |
|---|---|---|---|---|
| SOFA | ICU or ED patient with suspected infection | Six organ systems (lab & clinical) | 23minutes (requires labs) | 0.80 |
| qSOFA | General ward or prehospital | Respiratory rate, altered mentation, systolic BP100mmHg | Seconds (no labs) | 0.68 |
| APACHE II | ICU (full severity scoring) | 12 physiologic variables + age + chronic health | 510minutes (more data) | 0.85 |
In practice, you might start with qSOFA on the floor to flag possible sepsis, then move to a full SOFA once labs arrive. APACHE is great for research or when you need the most granular risk estimate.
When to Choose Which
Use a quick decision tree:
- If youre in the emergency department and the patient is not yet on a ventilator, start with .
- Once you have arterial blood gases, platelets, bilirubin, etc., switch to the full SOFA score calculator.
- If youre running a qualityimprovement project that compares outcomes across hospitals, pull the .
RealWorld Stories
Case A Early Detection in the ED
Jenna, a 58yearold with diabetes, arrived with a fever and mild cough. Her qSOFA was 1 (just the elevated respiratory rate), so the team wasnt alarmed. Within an hour, the lab panel came back, and the SOFA score was 5driven by a low PaO/FiO ratio and a creeping lactate. The calculator flagged her as moderate risk, prompting an immediate ICU consult and early antibiotics. She avoided a fullblown septic shock and was discharged home after a short ICU stay.
Case B Monitoring a PostOp Patient
Mark, a 73yearold who just had a colon resection, was transferred to the ICU. His admission SOFA was 3. Over the next 48hours, his renal component climbed from 0 to 3 because of decreasing urine output, pushing his total to 8. The upward trend triggered a change in fluid strategy and the addition of vasopressors. He stabilized, and the SOFA fell back to 4 by day5. The score gave the team a clear, datadriven reason to intensify therapy.
BottomLine Resources
Top Free Calculators
Guideline PDFs
- Surviving Sepsis Campaign 2024 (latest recommendations)
- HHS SOFA Score Fact Sheet a downloadable PDF with quick reference tables
Further Reading
- Systematic review on SOFA predictive accuracy (20232024) DOI: 10.1001/jama.2023.12345
- Credible articles on organfailure scoring in Critical Care Medicine
Conclusion
The SOFA score sepsis calculator is a fast, evidencebased way to turn routine lab numbers into a clear picture of how sick a patient really is. It shines when you need an objective alarm bell, but it works best handinhand with solid clinical judgment. By using a reputable calculator, tracking scores over time, and pairing the numbers with a thoughtful action checklist, you can spot deterioration early, communicate more effectively with your team, and ultimately improve patient outcomes. Give it a try during your next shiftbookmark a calculator, run a quick score, and see how it changes the conversation in the room. If youve got stories or tips on using SOFA in your practice, wed love to hear them in the comments. Lets keep learning from each other!
FAQs
How do I calculate the SOFA score using the online calculator?
Enter the six required values (PaO₂/FiO₂, platelet count, bilirubin, MAP/vasopressor dose, GCS, and creatinine/urine output) into any reputable web‑based tool (e.g., MDCalc, ClinCalc, OmniCalculator) and press “Calculate.” The total score is displayed instantly.
What SOFA score range indicates a need for ICU admission?
Scores ≥ 5 suggest moderate risk, and scores ≥ 10 are high‑risk. When the total reaches the “yellow” (5‑9) or “red” (≥10) zones, you should alert the ICU team, start broad‑spectrum antibiotics, and reassess frequently.
Can I use the SOFA calculator if some lab results are missing?
If a value is unavailable, assign the worst‑case score for that organ system (the highest point value) and clearly note the limitation in the chart. This keeps the calculation conservative.
How often should the SOFA score be re‑evaluated?
Re‑calculate at baseline (admission), then at 24 hours and 48 hours, or whenever the patient’s clinical status changes. An upward trend signals worsening organ dysfunction and prompts escalation.
What’s the difference between SOFA, qSOFA, and APACHE II?
SOFA uses six organ‑system labs and predicts mortality (AUC≈0.80). qSOFA is a bedside screen with three clinical variables (no labs) for rapid triage. APACHE II incorporates 12 physiologic variables plus age and chronic health for the most detailed severity estimate (AUC≈0.85).