Hey there! If youre scrolling through stacks of medical jargon looking for the best antibiotic for vomiting and diarrhea, youve landed in the right spot. Lets skip the fluff and give you the straightup info you need, whether youre dealing with a nasty bout yourself, caring for a child, or just curious. Grab a cup of tea, settle in, and lets figure this out together.
Quick Answer
If a bacterial infection is confirmed, azithromycin is currently the goto drug for most adults with vomiting and diarrhea. Fluoroquinolones (like ciprofloxacin or levofloxacin) and rifaximin are solid backups, while kids usually get a weightbased azithromycin dose or, in special cases, amoxicillinclavulanate.
Remember: antibiotics wont help a viral stomach bug. In those cases, hydration and rest are your best allies.
When Antibiotics Needed
What type of infection triggers vomiting+diarrhea?
Not every gastroissue needs a prescription. Heres the quick breakdown:
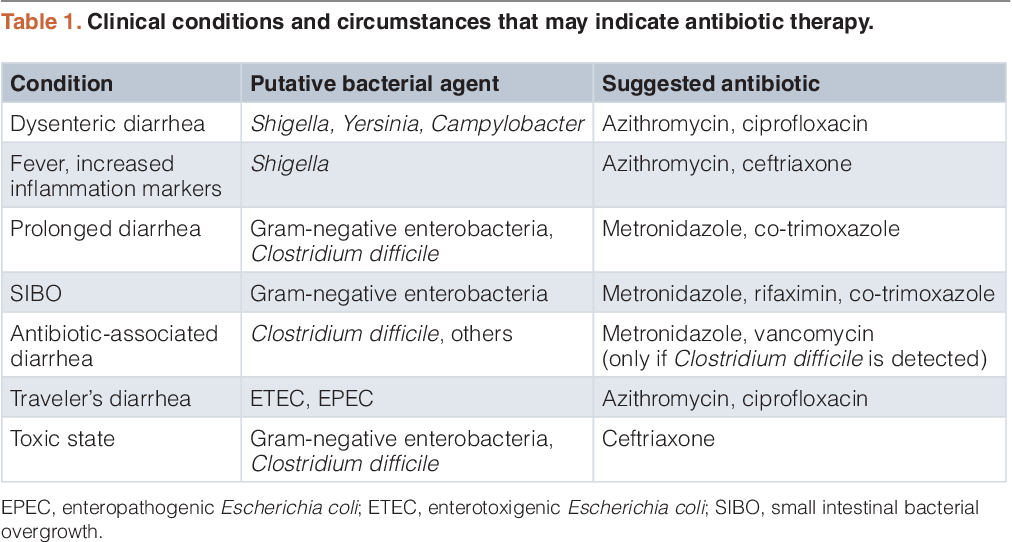
- Bacterial think Shigella, Campylobacter, invasiveE.coli, Salmonella. These are the culprits that truly respond to antibiotics.
- Parasitic such as Giardia. Often treated with metronidazole or tinidazole.
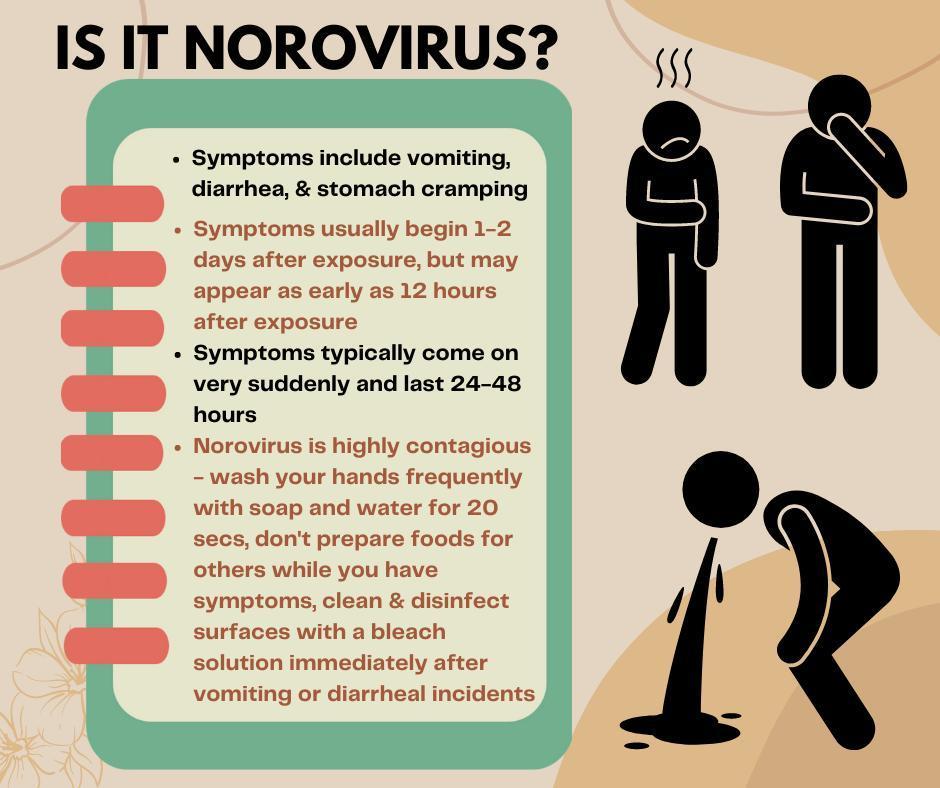
- Viral norovirus, rotavirus, adenovirus and heres the kicker: no antibiotics needed. Supportive care does the trick.
How do doctors decide to prescribe?
Clinicians weigh a handful of signals:
- Severity: High fever, blood in stool, or symptoms lasting more than three days.
- Dehydration risk: Especially in kids, older adults, or anyone with a compromised immune system.
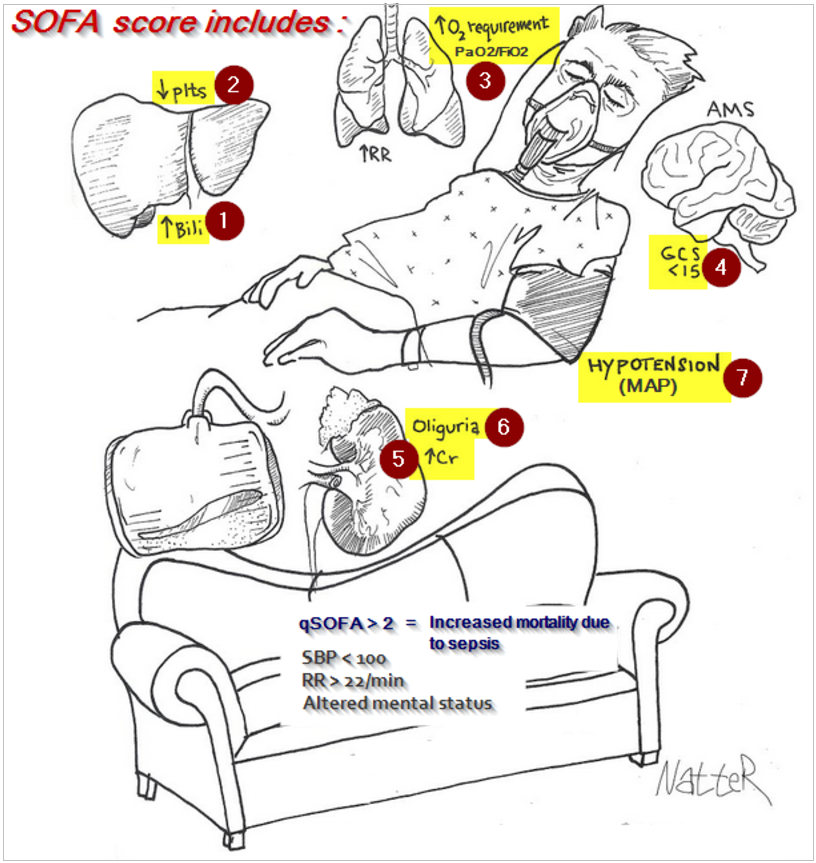
- Exposure history: Recent travel, outbreak alerts, or known contact with a bacterial source. If youre worried about how quickly an illness can progress to organ dysfunction, tools like the organ failure assessment can help clinicians evaluate severity in hospitalized patients.
When these red flags line up, the doctor will likely order a stool culture and, if bacterial, move forward with an antibiotic.
FirstLine Choices
Azithromycin the current gold standard
Why does azithromycin sit at the top of most guidelines?
- Broadspectrum coverage for the usual bacterial suspects.
- Simple dosing: One gram as a single oral dose for adults, or 10mg/kg once daily for three days in children.
- Good tissue penetration it reaches the gut lining where the infection lives.
According to the preferred firstline antibiotic for acute watery diarrhea and dysentery is azithromycin, thanks to its efficacy and lower resistance rates.
Fluoroquinolones ciprofloxacin & levofloxacin
These are the reliable plan B when azithromycin isnt an option (allergy, resistance, or local guidelines). Theyre especially handy for Salmonella and severe Campylobacter infections.
- Ciprofloxacin: 500mg orally twice a day for three days.
- Levofloxacin: 750mg once daily for three days.
Watch out for tendonitis warnings and photosensitivity and remember that fluororesistance is creeping up in parts of the world.
Rifaximin guttargeted option
If the culprit is a noninvasive diarrheagenic E.coli, rifaximin shines because it stays in the intestine and hardly enters the bloodstream, sparing you systemic sideeffects.
- Typical adult dose: 550mg three times a day for three days.
- Pediatric dose: 200mg three times a day for three days.
FirstLine Comparison Table
| Drug | Adult Dose | Pediatric Dose | Coverage | Main Sideeffects | Resistance Concerns |
|---|---|---|---|---|---|
| Azithromycin | 1g single oral dose | 10mg/kg daily 3days | Shigella, Campylobacter, invasiveE.coli | GI upset, QT prolongation | Low (macrolide resistance rising slowly) |
| Ciprofloxacin | 500mg bid 3days | 15mg/kg bid 3days | Salmonella, Campylobacter | Tendonitis, photosensitivity | Increasing fluororesistance |
| Levofloxacin | 750mg daily 3days | 10mg/kg daily 3days | Same as ciprofloxacin | Same as ciprofloxacin | Same as ciprofloxacin |
| Rifaximin | 550mg tid 3days | 200mg tid 3days | NoninvasiveE.coli | Mild nausea, flatulence | Minimal (poor systemic absorption) |
Other Effective Options
TrimethoprimSulfamethoxazole (TMPSMX)
In some regions, especially where Shigella prevalence is high, TMPSMX remains a firstline contender. Its a twoinone pill that attacks bacterial folicacid pathways.
Furazolidone & Metronidazole
Both have historic roots in treating bacterial and anaerobic infections. The NCBI textbook notes clinical cures within three days for certain gut infections when using these agents. Metronidazole shines for Clostridioides difficileassociated colitis, but only after confirming the infection.
When to Pair Antibiotics with Antidiarrheals
Travelers often ask if they can add loperamide to speed things up. The CDC yellow book says a single dose of loperamide 4mg, followed by 2mg after each loose stool (max 16mg/24h), is safe when combined with an appropriate antibiotic for travelers diarrhea.
Special Populations
Kids best antibiotic for vomiting and diarrhea in children
Children arent just small adults. Their metabolism and gut flora are different, so dosing matters:
- Azithromycin stays the top pick 10mg/kg as a single dose or split over three days.
- Fluoroquinolones are used only when benefits outweigh jointtoxicity risks.
- Avoid tetracyclines and chloramphenicol unless a specialist advises.
Pregnant & Breastfeeding Moms
Safety first! Azithromycin is classified as pregnancycategory B (generally safe). Fluoroquinolones cross the placenta and are best avoided.
Immunocompromised Adults
When the immune system is on a vacation, doctors may opt for broader agents, such as carbapenems, but only under specialist supervision. The risk of severe infection outweighs the risk of resistance in these cases.
Case Snapshot
Fouryearold Mia returned from a beach vacation with watery stools and frequent vomiting. After a quick pediatric visit, she received a weightbased azithromycin dose and oral rehydration salts. Within 48hours, her symptoms faded, and she was back to building sandcastles.
Safe Use Tips
Proper Dosing & Duration
Short courses work best. Most regimens last three days; extending beyond that usually offers no extra benefit and raises resistance risk.
Common Sideeffects & Warning Signs
- Stomach upset or mild rash often harmless.
- Allergic reactions (hives, swelling, trouble breathing) seek emergency care.
- Signs of C.difficile infection: persistent watery diarrhea after finishing antibiotics, accompanied by abdominal cramping.
Drug Interactions to Watch
Antacids can lower fluoroquinolone absorption, so separate them by at least two hours. Azithromycin may interact with warfarin, increasing bleeding risk always tell your doctor about other meds.
QuickReference Checklist (PrintFriendly)
- Confirm bacterial cause (stool culture, travel history).
- Choose firstline drug: azithromycin fluoroquinolone rifaximin.
- Weightadjust pediatric doses.
- Hydrate aggressively (ORS, clear fluids).
- Finish the full course, even if you feel better.
- Monitor for severe sideeffects; call a clinician if they appear.
Frequently Asked Questions
What is the best antibiotic for gastroenteritis?
Azithromycin is the preferred firstline therapy for bacterial gastroenteritis that causes both vomiting and diarrhea, with fluoroquinolones and rifaximin as effective alternatives.
Can I use antibiotics for viral stomach flu?
No. Viral gastroenteritis (like norovirus or rotavirus) does not respond to antibiotics. Supportive carefluid replacement and restis the correct approach. To reduce the chances of catching or spreading viral causes, learn how to prevent stomach flu through hygiene and isolation measures.
Is it safe to give antibiotics to a child with diarrhea?
Only when a bacterial cause is strongly suspected. Azithromycin at 10mg/kg is the most studied pediatric option; fluoroquinolones are reserved for rare, severe cases.
When should I see a doctor?
If you have a fever over 101F, blood in your stool, dehydration signs (dry mouth, dizziness), symptoms lasting more than three days, or you belong to a highrisk group (children, pregnant, immunocompromised), get medical help promptly.
Do I need a prescription for azithromycin?
Yes, in most countries azithromycin is prescriptiononly. Selfmedicating can lead to resistance or misuse, so always involve a healthcare professional.
Sources & Further Reading
To keep this guide trustworthy, we consulted several reputable sources:
- PMCID5650106 Antibiotic Therapy for Acute Watery Diarrhea and Dysentery.
- Medscape Bacterial Gastroenteritis Medication guidelines.
- NCBI Book Antibiotic therapy for diarrhea & vomiting.
- CDC Yellow Book Travelers diarrhea recommendations.
- Mayo Clinic Viral gastroenteritis overview.
Takeaway: When vomiting and diarrhea stem from a bacterial infection, azithromycin is usually the best pick, with fluoroquinolones and rifaximin as solid backups. Children and special groups need dose tweaks and extra caution. Always confirm the cause, stay hydrated, and finish the full course. Got your own story or lingering question? Share it in the commentslets help each other feel better!
FAQs
When should I consider taking an antibiotic for vomiting and diarrhea?
Antibiotics are only recommended if a bacterial cause is likely—signs include high fever, blood in stool, symptoms lasting more than three days, or a recent travel/outbreak exposure.
Is azithromycin safe for children with gastroenteritis?
Yes. Azithromycin is the preferred pediatric option, given as a weight‑based dose (10 mg/kg once daily for three days) and has a good safety record in children.
Can fluoroquinolones be used during pregnancy?
Fluoroquinolones (ciprofloxacin, levofloxacin) cross the placenta and are generally avoided in pregnancy; azithromycin (category B) is the safer alternative when an antibiotic is needed.
What are the common side‑effects of the antibiotics used for vomiting and diarrhea?
Typical side‑effects include mild stomach upset, rash, and, for azithromycin, possible QT‑interval prolongation. Fluoroquinolones can cause tendonitis and photosensitivity, while rifaximin may lead to flatulence.
How long should the antibiotic course last for acute bacterial diarrhea?
Most regimens are short—usually three days. Extending treatment beyond this offers little extra benefit and increases the risk of resistance.