Quick Answer Intro
What are antibiotics for colitis treatment and when should they be used?
Antibiotics are medicines that kill or stop the growth of bacteria. In colitis, theyre most helpful when the inflammation is caused by an infection (likeClostridioidesdifficile) or when a bacterial overgrowth is adding fuel to an existing inflammatory bowel disease (IBD) flare. In those cases, a short, targeted course can bring relief and prevent complications. Patients looking into adjunct approaches for IBD may also consider lifestyle and supplement options; for trusted product guidance, see resources on ulcerative colitis supplements.
Key takeaway
Antibiotics are not a blanket cure for every colitis episode. They work best for infectious colitis and as an adjunct for certain ulcerative colitis or Crohns disease flares where bacteria are suspected.
Why Antibiotics Matter
Which types of colitis might need antibiotics?
Not all colitis is created equal. Heres a quick snapshot of the main categories where antibiotics often enter the picture:
- Infectious colitis bacterial invaders such asCampylobacter,Salmonella, orC.difficile.
- Pseudomembranous colitis a severe form of C.difficile infection.
- Ulcerative colitis with secondary bacterial overgrowth when the gut flora gets out of balance during a flare.
- Crohns disease complications like intraabdominal abscesses where an oral regimen wont reach the infection.
What does the evidence say?
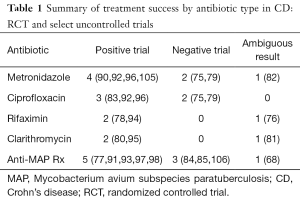
Studies published in reputable journals (e.g., ) show that a combination of ciprofloxacin and metronidazole tops the list for broadspectrum bacterial colitis, while vancomycin remains the gold standard for C.difficile. For gutrestricted issues, rifaximin has shown modest benefit and carries minimal systemic sideeffects.
Best Choices Guide
Whats the best antibiotic for colitis?
Choosing the best drug depends on the underlying cause. Below is a quick cheatsheet you can keep on hand. The table also highlights the typical dose, treatment length, and why each option is preferred.
| Scenario | FirstLine Antibiotic(s) | Typical Dose & Duration | Why Its Preferred |
|---|---|---|---|
| C.difficile colitis | Vancomycin (oral) Fidaxomicin | 125mg q6h for 10days | High cure rate, stays in colon where its needed |
| Communityacquired bacterial colitis | Ciprofloxacin+Metronidazole | 500mg BID + 500mg TID, 710days | Covers gramnegative bugs and anaerobes |
| IBD flare with suspected bacterial overgrowth | Rifaximin (nonsystemic) | 550mg BID, 714days | Minimal systemic absorption, fewer sideeffects |
| Severe ulcerative colitis needing IV therapy | Ampicillin+Gentamicin+Clindamycin (IV) | Weightbased dosing, 57days | Rapid bactericidal action for hospitalized patients |
Is Augmentin ever used?
Augmentin (amoxicillin/clavulanate) shows up in a few older case reports, but modern guidelines (see the ) advise against it as a firstline agent because it can disturb the gut microbiome further and increase the risk of C.difficile recurrence.
Which antibiotics should ulcerative colitis patients avoid?
Broadspectrum drugs like tetracycline, highdose amoxicillin, or prolonged macrolide courses are generally discouraged unless a specific infection is proven. They can aggravate dysbiosis, making flareups harder to control.
Treatment Duration Details
How long should I stay on antibiotics for colitis?
Duration varies by the infections severity and the drug used:
- Infectious bacterial colitis: 714days; youll usually finish the course even if you feel better early to prevent resistance.
- C.difficile: 10days for mildmoderate disease, up to 14days for severe cases.
- IBD adjunct therapy: 24weeks, followed by a reassessment with your gastroenterologist.
When is it okay to stop early?
Only if you experience serious sideeffects (like a severe rash, persistent nausea, or kidney issues) and after discussing it with your doctor. Stopping a course too soon can lead to bacterial rebound and resistance.
Risks & SideEffects
What are the common sideeffects?
Every antibiotic class carries its own personality quirks:
- Fluoroquinolones (ciprofloxacin): tendon pain, QTprolongation, possible gutflora disruption.
- Nitroimidazoles (metronidazole): metallic taste, occasional neuropathy if you stay on it longer than two weeks.
- Glycopeptides (vancomycin IV): kidney toxicity and hearing loss (rare, mostly with IV use).
How can I keep the risks low?
Here are some practical, friendtofriend tips:
- Take the medication with food unless the label says empty stomach. It can spare your stomach lining.
- Stay wellhydrated water helps flush metabolites and reduces kidney strain.
- Keep a medication journal. Jot down the start date, dose, and any quirks you notice. This makes followup appointments smoother.
- Watch for redflag symptoms: persistent watery diarrhea, fever, or severe abdominal pain could signal a new infection or a complication.
Real World Stories
A short story: When ciprofloxacin saved my summer
Last July I took a backpacking trip through Southeast Asia. Two days after a streetfood feast, I was hit with cramping, fever, and explosive diarrhea. My doctor, after a quick stool test, prescribed ciprofloxacin plus metronidazole. Within 48hours the worst of the cramps disappeared, and I was back exploring night markets. The lesson? Targeted antibiotics can knock out the nasty bacteria fast, but you still need to stay hydrated and finish the whole pack.
Clinician insight: Why I reserve vancomycin for C.difficile
Dr. Elena Morales, a gastroenterology fellow at a major academic center, explains: Vancomycin stays largely in the colon, which is exactly where C.difficile lives. Oral fidaxomicin is another excellent option, but its pricier. I reserve vancomycin for the first line because the evidence (see the ) shows a >90% cure rate when used correctly.
Guidelines & Resources
Where do the official recommendations come from?
For trustworthy, uptodate advice, lean on these bodies:
- IDSA/SHEA 2024 C.difficile guideline the goto for vancomycin and fidaxomicin dosing.
- ECCO 2023 IBD Management Guidelines outline when antibiotics are appropriate in ulcerative colitis and Crohns disease.
- Crohns &Colitis Foundation fact sheets (2025) easytoread PDFs that list safe antibiotics for ulcerative colitis patients.
How can you stay current?
Subscribe to the Foundations newsletter, set up alerts on clinical decision apps like UpToDate or Lexicomp, and bookmark reputable sites (Mayo Clinic, Medscape) for dose calculators and druginteraction checkers.
Bottom Line Summary
Antibiotics are powerful, but theyre a precise tool, not a blanket fix. When you have infectious colitis, or when a bacterial overgrowth is fueling an IBD flare, the right drugwhether its vancomycin, ciprofloxacin+metronidazole, or rifaximincan bring rapid relief. At the same time, respecting treatment duration, monitoring sideeffects, and avoiding unnecessary broadspectrum agents protects both your gut and the wider community from resistance.
So, before you reach for the nearest pill bottle, have a candid conversation with your gastroenterologist. Share any recent antibiotics youve taken, list the meds youre on, and ask which regimen aligns with your specific type of colitis. If youve navigated this terrain before, wed love to hear your storydrop a comment below or join the discussion in our community forum. Together, we can make sense of the science while keeping the conversation warm, real, and supportive.
FAQs
When are antibiotics necessary for colitis treatment?
Antibiotics are used primarily when colitis is caused by bacterial infections such as Clostridioides difficile or when bacterial overgrowth worsens inflammatory bowel disease flares.
Which antibiotics are preferred for treating C. difficile colitis?
Oral vancomycin is the first-line antibiotic for C. difficile colitis, often dosed at 125 mg every 6 hours for 10 days. Fidaxomicin is another option but tends to be more expensive.
Can antibiotics help in ulcerative colitis flares?
Antibiotics like rifaximin may be used as adjunct therapy in ulcerative colitis flares suspected to involve bacterial overgrowth, but they are not a cure for ulcerative colitis itself.
What are common side effects of antibiotics used to treat colitis?
Side effects vary by antibiotic class but can include gastrointestinal upset, metallic taste, neuropathy (with metronidazole), tendon pain (with ciprofloxacin), and rare kidney toxicity (with vancomycin).
How long should antibiotic courses for colitis last?
Treatment duration varies: infectious colitis generally requires 7-14 days, C. difficile colitis around 10 days (extended to 14 for severe cases), and IBD-related bacterial overgrowth may need 2-4 weeks with reassessment.