Most people dont realize that asthma antibody therapy can cut severe attacks by up to 60% in the right patients and it does so without wiping out the whole immune system. Below youll find a straighttothepoint guide that explains the key drugs, how they work, the risks, the cost, and what questions you should ask your doctor.
Why Biologics Matter
What makes asthma antibody therapy different?
Traditional inhalers and oral steroids fight the symptoms of asthma, but they dont target the underlying inflammation that fuels frequent flareups. Biologics are labcrafted monoclonal antibodies that lock onto specific molecules driving that inflammation, essentially turning off the alarm before it wakes you up at night.
Who is a candidate for these treatments?
Guidelines (according to the ) suggest biologic therapy for adults and teens who:
- Have at least2exacerbations a year despite highdose inhaled corticosteroids (ICS) and a longacting betaagonist (LABA).
- Show elevated biomarkers such as blood eosinophils (>150300cells/L) or high IgE levels.
- Struggle with oral corticosteroid dependence.
If you tick those boxes, a conversation with a pulmonologist can open the door to a personalized biologic plan. For individuals managing complicated airway diseases, maintaining effective cystic fibrosis airway clearance is equally critical for long-term lung health and minimizing recurrent flare-ups.
Monoclonal Antibodies List
| Drug (Brand) | Target | Approved Year | Typical Use |
|---|---|---|---|
| Omalizumab (Xolair) | IgE | 2003 | Allergic asthma |
| Mepolizumab (Nucala) | IL5 | 2015 | Eosinophilic asthma |
| Benralizumab (Fasenra) | IL5R | 2017 | Eosinophilic asthma |
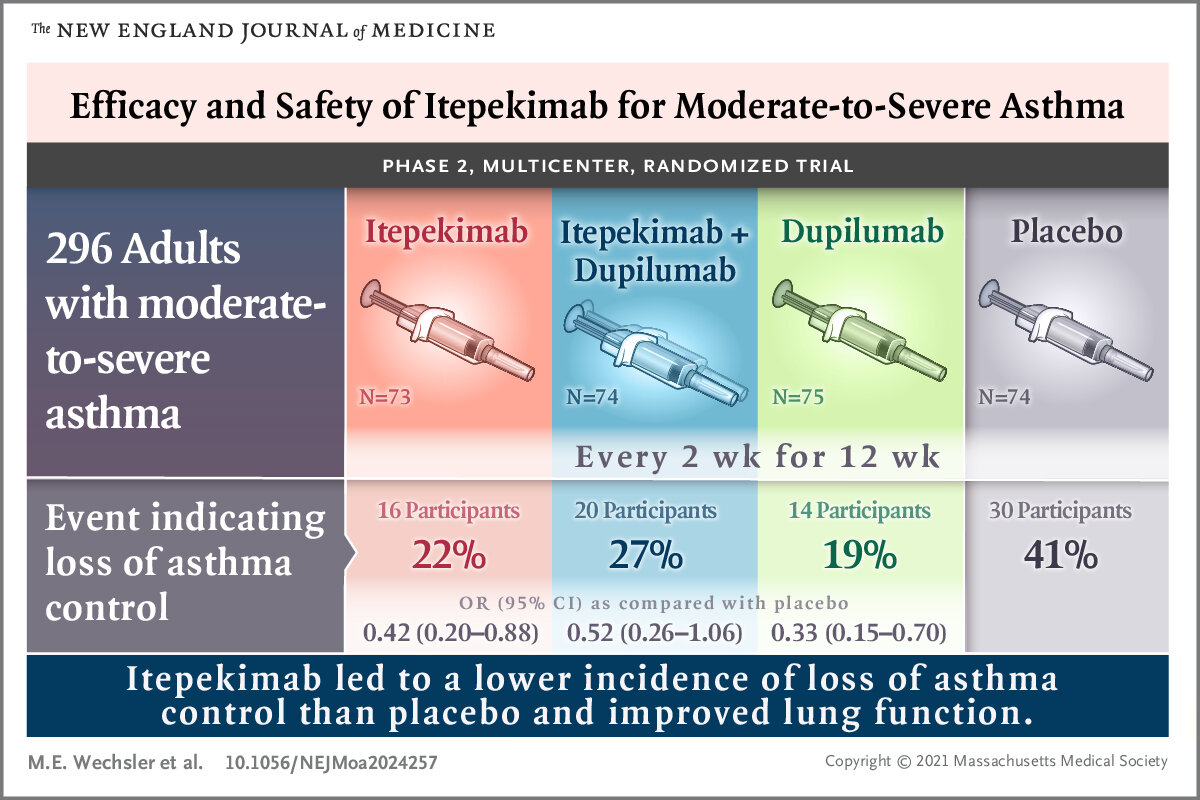
| Dupilumab (Dupixent) | IL4R (IL4/IL13) | 2018 | Type2 inflammatory asthma |
| Tezepelumab (Tezspire) | TSLP | 2022 | Broad severe asthma |
| Reslizumab (Cinqair) | IL5 | 2016 | Eosinophilic asthma (IV) |
How do I pick the right one?
Think of each antibody as a key that fits a specific lock:
- If your labs show high IgE, omalizumab is the goto.
- If eosinophils dominate, mepolizumab, benralizumab, or reslizumab are worth a look.
- When you need a broader approach that covers multiple pathways, tezepelumab (the newest kid on the block) has shown impressive results.
How Antibodies Work
Can you explain the science in plain English?
Imagine your airway inflammation as a wild house party. Certain guests (IgE, IL5, IL4, TSLP) keep the music loud and the lights flashing. Monoclonal antibodies act like bouncers who recognize those troublemakers and escort them out, letting the airways calm down and breathe easier.
What pathways are blocked?
- IgE targeted by omalizumab
- Interleukin5 (IL5) blocked by mepolizumab, benralizumab, reslizumab
- IL4/IL13 inhibited by dupilumab
- Thymic stromal lymphopoietin (TSLP) neutralized by tezepelumab
Benefits & Efficacy
How much can these drugs reduce attacks?
Clinical trials consistently show a 3070% drop in severe exacerbations, depending on the molecule. For example, a large reported a 71% reduction with tezepelumab, while omalizumab typically trims attacks by about 35%.
Do they improve daily life?
Patients often report higher Asthma Control Test (ACT) scores, fewer nighttime awakenings, and a reduced need for oral steroids. One realworld story: Maria, a 42yearold teacher, cut her oral corticosteroid use by 90% after switching to dupilumab and now enjoys a normal workday without the constant fear of a sudden attack.
Risks & Side Effects
What are the common asthma injection side effects?
| Side Effect | Frequency | Notes |
|---|---|---|
| Injectionsite pain/redness | Common (2030%) | Usually mild, resolves in a day |
| Headache | Occasional (1015%) | Often transient |
| Upperrespiratory infections | Rare (5%) | More reported with tezepelumab |
| Allergic reactions / anaphylaxis | Very rare (<0.1%) | Omalizumab carries the highest warning label |
Are there drugspecific concerns?
Yes. Omalizumab can trigger anaphylaxis, so patients receive the first few doses in a medical setting. Benralizumab depletes eosinophils, which may raise questions for people with parasitic infection risk. Tezepelumab has shown a slightly higher rate of nasopharyngitis, but overall its safety profile is reassuring.
What does longterm safety look like?
Postmarketing surveillance up to five years (as reported by the ) shows no unexpected organ toxicity. Most concerns revolve around injection reactions and rare allergic events, which are manageable with proper monitoring. In patients with complex lung conditions, understanding airway clearance methods can further support optimal respiratory health alongside biologic therapies.
Cost & Access
How much does biologic therapy for asthma cost?
In the United States, annual prices range from$30,000to$45,000, while the United Kingdoms NHS typically negotiates lower prices, around20,00030,000 per year. Canada, Australia, and many European nations have similar ballpark figures, adjusted for local healthcare budgets.
What helps cover the price?
Insurance plans (Medicare PartB, private carriers) often cover a large portion of the cost after prior authorization. In the UK, the NHS specialty commissioning pathway handles access, and Australias PBS (Pharmaceutical Benefits Scheme) subsidizes the majority of the expense for eligible patients.
Does the route of administration affect cost?
Selfadministered subcutaneous injections (omalizumab, dupilumab, tezepelumab) tend to lower clinicvisit costs, while intravenous infusions like reslizumab require infusioncenter resources, adding to overall expense.
Choosing the Right Option
Which antibody fits my profile?
| Patient Profile | Preferred Biologic | Why |
|---|---|---|
| High IgE, allergic triggers | Omalizumab | Directly neutralizes IgE |
| Eosinophils>300cells/L | Mepolizumab / Benralizumab | Blocks IL5 pathway |
| Mixed phenotype, wants broad coverage | Tezepelumab | Targets upstream TSLP, works for many endotypes |
| Concurrent atopic dermatitis | Dupilumab | Blocks IL4/IL13, helps skin and lungs |
What should I ask my doctor?
- What biomarker results support a specific antibody?
- Will I need a premedication before injections?
- How will this affect my current inhaler regimen?
- What is the expected timeline for seeing improvement?
- Are there assistance programs to offset the cost?
RealWorld Stories
Can patients really feel the difference?
John, a 55yearold exsmoker, recalls his first year on benralizumab: I used to carry a rescue inhaler everywhere. After a few months, I could go a whole week without even thinking about it. My wife finally stopped waking me up at 2a.m. with a wheeze.
These anecdotes echo data from the , where 78% of respondents reported significant improvement after starting a biologic. For people who also manage cystic fibrosis, striking a balance between medications and daily infection controlsuch as diligent cf social distanceremains a crucial component of living well with chronic lung conditions.
Future Directions
Whats on the horizon?
Researchers are now exploring upstream cytokines like IL33 and IL25, as well as oral smallmolecule inhibitors that could someday replace injections. Geneediting trials are in early phases, aiming to correct underlying immune dysregulation before severe asthma even manifests.
How might these advances change cost and access?
If oral agents prove effective, we could see a drop in administrationrelated expenses and broader insurance coverage. Until then, the current biologic arsenal remains our most potent tool for taming severe disease.
Asthma antibody therapy has turned a oncedevastating condition into a manageable one for many patients. The key is understanding the benefits, the risks, and the financial landscape, then working handinhand with a specialist to pick the right fit. If youre curious about whether a biologic could change your life, download our quickcheck questionnaire, talk to your doctor, and take the first step toward breathing easier.
FAQs
What is asthma antibody therapy and how does it differ from inhalers?
Asthma antibody therapy uses monoclonal antibodies that target specific immune molecules (IgE, IL‑5, IL‑4/13, TSLP) driving airway inflammation, whereas inhalers mainly deliver steroids or bronchodilators to treat symptoms.
Who is eligible for biologic treatment?
Patients with ≥2 severe exacerbations a year despite high‑dose inhaled steroids + LABA, elevated eosinophils or IgE, or dependence on oral steroids are typical candidates.
How quickly can I expect improvement after starting a biologic?
Most people notice fewer night‑time symptoms and rescue inhaler use within 2‑3 months; full reduction in severe attacks often appears after 4‑6 months of consistent therapy.
What are the most common side effects of asthma antibodies?
Injection‑site reactions, headache, and mild upper‑respiratory infections are common; rare events include anaphylaxis (mainly with omalizumab) and eosinophil depletion concerns with benralizumab.
Will my insurance cover the cost of these biologics?
Many plans (Medicare Part B, private insurers, NHS, PBS) require prior authorization but typically cover a large portion after approval; patient‑assistance programs can further offset out‑of‑pocket costs.